Several classes are used to treat inflammation: NSAIDS, steroids, biologics (target chemical pathways of inflammation), cancer drugs (strong anti-inflammatory properties.
Steroids have stronger anti-inflammatory functions than NSAIDS, however, chronic NSAIDs are safer than long term use of steroids.
Steroids can be used for a variety of conditions: inflammatory (rheumatoid arthritis, psoriasis, asthma flare-up), immune suppression (e.g transplant), adrenal insufficiency (replace our endogenous steroids which the adrenal gland is not producing enough amount).
Two primary endogenous steroids: cortisol (can be replaced by any steroids), aldosterone (replace by fludrocortisone).
Two types of steroids: glucocorticoids and mineralocorticoids.
Cushing’s syndrome Vs. Addison’s disease
Cushing’s: Adrenal gland produces too much cortisol, or too much exogenous steroid intake, higher than what the body normally produces.
Symptoms: similar to steroids side effects, fat deposit in face, glaucoma, acne, psychiatric changes, GI bleeding/ulcers, pink/purple stretch mark/bruise easily, diabetes, growth retardation, hirsutism (women only), infection, slow wound healing.
Reduce systemic steroid risks: alternate day dosing, initial high dose to reduce inflammation the taper down to treat remaining inflammation, use localized forms instead: joint injection, suppository (Encocort EC), inhaled steroids (ICS).
Addison’s: The adrenal gland does not make enough cortisol, or when high dose exogenous steroids are discontinued suddenly, which can cause an Addisonian crisis.
Mineralocorticoid
Drug: Fludrocortisone.
MOA: mimics aldosterone and has mineralocorticoid activity, which maintains a balance of sodium and water, which keeps BP stable. (“mineral” = minerals such as Na)
Indication: Addison’s disease, and off label use for orthostatic hypotension.
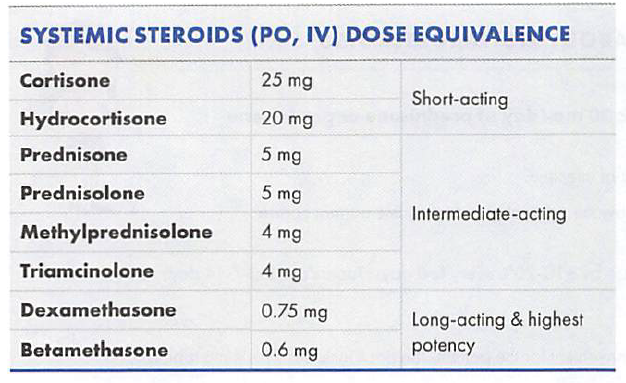
Notice that fludrocortisone does not even show up in the potency chart, because it is not usually used for anti-inflammation.
MOA: ↑ blood glucose & hydrolysis of fats from adipocytes (think the body needs energy from glucose and fat).
Short term SE: GI, mood swing, insomnia, fluid retention (can ↑ BP), ↑blood glucose, ↑appetite/weight gain; Long term SE: Cushing’s syndrome. “gluco” think about alternation in glucose levels.
Warnings: adrenal suppression (must taper slowly if taking longer than 14 days), immunosuppression, high dose/chronic therapy is contraindicated with live vaccine, and serious infections.
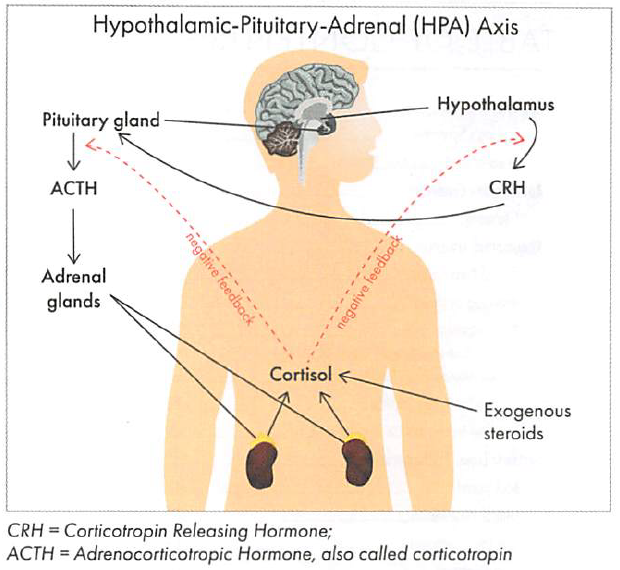
Systemic steroids have more glucocorticoid activity and anti-inflammatory effects. They cause adrenal gland to stop producing endogenous cortisol due to feedback inhibition. This is called the suppression of hypothalamus-pituitary-adrenal (HPA) axis.
Long term steroids need to be taper off to allow adrenal gland time to resume cortisol production.
Cortisone is a prodrug of cortisol, prednisone is prodrug of prednisolone (commonly used in children).
Autoimmune disorders
Body’s immune system is impaired and attacks its own healthy tissue.
Common symptoms: fatigue, weakness, and pain.
Labs in detecting inflammation: C-reactive protein (CRP), rheumatoid factor (RF), erythrocyte sedimentation rate (ESR), and anti-nuclear antibody (ANA).
Examples: psoriasis, Rheumatoid arthritis (RA), multiple sclerosis (MS), celiac disease, systemic lupus erythematosus (SLE), Sjogren’s syndrome, Raynaud’s syndrome, type I DM, Hashimoto and Graves’ disease.
Treatment
Immunosuppressants: Drugs that suppress the immune system which can ↓ immune response.
However, strong immune suppression can ↑ risk of: infections including reactivation of TB/hepatitis, lymphomas/certain skin cancers, unable to get live vaccines (unless prior to immunosuppressive therapy).
Multiple sclerosis (MS)
MS is believed to be an immune-mediated disease of the central nervous system (CNS) where the body's own defenses attack the fatty myelin sheath that surrounds/protects nerve fibers. The end result of T-cell and B-cell activity is nerve fiber scarring (or sclerosis), and interruption of nerve signals traveling to/from the brain and spinal cord. MS is chronic with progressive physical disability.
The interruption of nerve impulses results in a variety of neurologic symptoms: blurred vision, loss of balance/poor coordination poor memory, spasticity, weakness, numbness, tremor, tingling, dizziness, fatigue; No two patients experience the same course of disease.
There is no cure for MS and treatment goal is to delay progression. Immunomodulating agents may slow progression by reducing the frequency and severity of relapses.
Disease-modifying agents
Glatiramer acetate (Copaxone)
MOA: amino acid polymers activate T-cells that suppress the cells attaching myelin.
It’s the only preg cat B amongst the disease-modifying therapies for MS.
20mg SC daily or 40mg SC 3x/week, refrigerate, can warm in room temp 30 mins before injection to reduce injection site reaction.
Interferon-beta 1a ((Avonex and Rebif) and 1b (Betaseron and Extavia):
MOA: antiviral and antiproliferative effects
well-established for relapsing forms of MS, start low and titrate up to target dose.
The long-acting pegylated 1a has the advantage of SC every 14 days instead of weekly or TIW, QOD, therefore better tolerated than other interferons.
SE: flu-like symptoms
dimethyl fumarate (Tecfidera)
an oral option for relapsed forms of MS, it seems to protect neurons and myelin and has anti-inflammatory properties.
SE: GI events (NVD, abdominal pain, dyspepsia), flushing (premediate with ASA, take with food), ↑WBC.
teriflunomide (Aubagio)
an oral option for relapsed forms of MS, it is an active metabolite of leflunomide, an immunomodulator used in RA to slow down the disease progression.
Don’t be surprised to see leflunomide being used in place of Aubagio, it’s cheaper although hasn’t been studied in MS.
Teratogenic: It takes 2 years for the drug to be completely out of the system, should wait to get pregnant, or use wash out treatment with activated charcoal or cholestyramine.
boxed warning of hepatoxicity.
fingolimod (Gilenya oral caps)
MOA: It's a sphingosine 1-phosphate receptor modulator that prevents the movement of lymphocytes from the lymph nodes to CNS.
the first oral disease-modifying MS agent.
warnings: macular edema ("len" in Gilenya), avoid live vaccines 2 months after Gilenya, causes lots of heart problems (first dose must be given in a medical office because profound ↓in HR, avoid QT-prolonging drugs)
CI in recent cardiovascular events, monitor BP, HR, and ECG.
natalizumab (Tysabri)
MOA: monoclonal antibody with anti-inflammatory effects (works by preventing the adhesion of endothelial cells with immune cells, which stops immune cells from entering the CNS).
SE: ↑ risk of infection.
Enroll in the TOUCH program due to boxed warning of PML (progressive multifocal leukoencephalopathy, a very serious brain condition): only administered at an infusion center, MRI.
Other monoclonal antibody therapies: alemtuzumab (Lemtrada, Campath)
Mitoxantrone (Novantrone)
A Chemotherapy that can treat multiple sclerosis (MS), reserved for rapidly worsening disease with persistent inflammations. It can also treat prostate cancer and certain types of leukemia.
SE limits the use of mitoxantrone: cardiotoxicity (turns everything blue: hypoxia).
Acute flare-ups of MS
Mainstream is high dose corticosteroids: Methylprednisolone, betamethasone, prednisolone, triamcinolone.
Common regimen: Methylprednisolone IV or PO x 3-5 days, followed by taper (up to 3 weeks)
Other autoimmune diseases
Celiac Disease (celiac sprue): An immune response in the small intestine to gluten, chronic inflammation leads to damage of the small intestine's lining and prevents absorption of nutrients. Caution for drugs that are gluten-free, excipients may not be.
Raynaud’s Phenomenon: triggered by exposure to cold and/or emotional stress, which causes vasospasm in the extremities; Skin turns white then to blue fingers and toes. When warmed, painful swelling can occur in hands and feet. Drug of choice: calcium channel blockers (for their peripheral vasodilatory effect).
Drug-induced Lupus Erythematosus (DILE): procainamide is the most common drug that causes this, hydralazine (alone and in BiDil).
Sjogren's Syndrome: most often characterized by severe dry eyes (artificial teardrops 1st line, cyclosporine [Restasis] for patients who still do not get satisfactory) and dry mouth (Cholinergic drugs would produce saliva, pilocarpine [Salagen], cevimeline [Evoxac]).
Quiz
Which of the following is a black box warning for use of peginterferon alpha-2b injection? (Select ALL that apply.)
Fatal thrombocytopenia
Fatal neuropsychiatric disorders
Fatal auto-immune disorders
Fatal infectious disorders
Fatal ischemic disorders
What is recommended as a first-line for newly diagnosed multiple sclerosis?
Betaseron
Oral prednisone
Natalizumab
Methylprednisolone
Rebif + mitoxantrone
Which of the following counseling points is correct when dispensing an interferon injectable prescription for multiple sclerosis?
Apply heat to the injection site before and after to reduce injection site pain.
If the medication cannot be used within 1 month, freeze the syringe to allow beyond-date use.
Use same injection site each time.
NSAIDS may reduce flu-like symptoms
If the medication reaches room temp, it is no longer active and should be discarded.
What is thought to be the cause of the symptoms associated with MS?
Hyperexcited nerve fibers
Myelin sheath damage
Neuronal overgrowth
Serotonin level imbalance
Which symptoms would most likely lead to a diagnostic workup for MS?
Numbness, blurred vision, and fatigue
Memory loss, depression, anxiety
Confusion, excessive thirst, bruising
Shortness of breath, palpitations, dizziness
What is the typical treatment goal for a patient with MS?
Delay disease progression
Cure
Heal nerve damage
Reverse disability
You are counseling a patient on the common side effects of glatiramer acetate therapy. Which side effect should you mention?
Low WBC
Injection site reactions
Progressive multifocal leukoencephalopathy (PML)
Post-injection reactions
Ashley is 36 years old and was diagnosed with relapsing-remitting MS (RRMS) 2 years ago. She was started on interferon beta-1a and has been doing well, but now she’s complaining of muscle tightness in her legs. What do you recommend for Ashley’s spasticity symptoms?
Tizanidine
Mirtazapine
Propranolol
Amantadine
It’s been 3 years and your patient Ashley, who has since been switched to teriflunomide, had been doing well, but had a flare-up about 6 months ago. She’s been battling with “feeling blue” and is having a hard time getting motivated to get out of bed in the morning ever since. She reports burning, tingling pain from time to time in her hands and feet. What do you recommend for Ashley’s symptoms?
Dalfampridine
Baclofen
Duloxetine
Fluoxetine
Answers
Peginterferon alpha-2b injection has a boxed warning for fatal neuropsychiatric, autoimmune, infectious, and ischemic disorders. Patients should be closely monitored.
Interferons (Betaseron, Avonex, and Rebif) and glatiramer acetate are considered first-line disease-modifying drugs (DMDs) for the treatment of MS. Natalizumab is reserved for patients who do not respond to traditional therapy. As the disease progresses, treatment with DMD + mitoxantrone pulse therapy may be used. Corticosteroids are the cornerstone for acute exacerbations but play no role in treating the disease itself.
Acetaminophen or NSAIDs may reduce flu-like symptoms associated with the interferon injections. The injections for multiple sclerosis should never be frozen and should always be protected from light. To ease injection pain, apply ice, not heat, and the injection site should be rotated each time. It is ok to allow the injectable to reach room temperature prior to the injection to ease the injection site pain.
Myelin sheath damage.
Numbness, blurred vision, and fatigue
Slow the progression, MS can not be cured.
Injection site reactions.
A, tizanidine (Zanaflex) is used for muscle spasm relief.