Last updated on: March 25th, 2018
Background
- Reduced blood flow to penis
- Common causes and contributors: vascular supply compromise and atherosclerosis (DM, HTN, heart disease, nerve damage), obesity, BPH, urinary incontinence, hormone imbalance, psychological problems, androgen deficiency (testosterone therapy has been associated with an increased risk of CV complications)
Avoid these offending drugs
- BP meds: diuretics (spironolactone exhibits hormonal imbalance to suppresses testosterone mediated libido), CCB (nifedipine, verapamil), ACEI (captopril, enalapril), centrally acting agents (guanfacine, clonidine, methyldopa), ββ (metoprolol, propranolol, atenolol): decreased intravascular volume or diminished arteriolar flow to penis.
- Antipsychotic: haloperidol, chlorpromazine, fluphenazine, thioridazine, 1st and 2nd genre are reported to cause ED, retrograde ejaculation, sexual dysfunction
- Antidepressant: SSRI, TCA (anticholinergic actions), bupropion, lesser with SNRI
- Antihistamines (dimenhydrinate, hydroxyzine, meclizine, diphenhydramine) and other anticholinergics (for more detailed review see chapter on overactive bladder)
- BPH: finasteride, silodosin, urinary incontinence drugs
- Chemo drugs: decrease sex hormones, leuprolide (Lupron)
- Cimetidine: block androgenic hormone, androgen is known to play a role in achieving an erection.
- Opioid: esp. methadone
- Nicotine
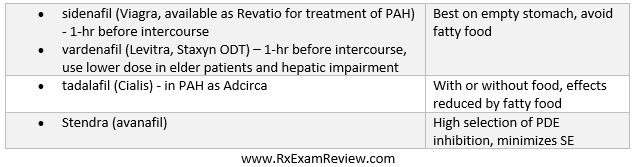
PDE5 inhibitor
- MOA: A phosphodiesterase type 5 inhibitor (PDE5 inhibitor) is a drug used to block the degradative action of cGMP-specific phosphodiesterase type 5 (PDE5) on cyclic GMP in the smooth muscle cells lining the blood vessels supplying the corpus cavernosum of the penis.
- Because PDE5 receptors also present in the arterial wall smooth muscle within the lungs, PDE5 inhibitors were originally used for the treatment of pulmonary artery hypertension - PAH. Erectile was discovered as a side effect of these drugs
- SE: class effect of vasodilation (HA, flushing, sudden drop in BP, dizziness), vision loss, priapism, loss of hearing
- Absolute CI with street drug nitrates: amyl nitrate, butyl nitrate (“popper”) – may reduce BP to a dangerous level
- DDI: If patient has angina, avoid NTG 24-hr after sidenafil/vardenafil, 48-hr after tadalafil
- Caution use with alpha blocker therapy, use a selective agent like tamsulosin, silodosin (Rapaflo) instead of non-selective agents (terazosin, doxazosin).
- Drugs
Alternative agent
- Intracavernosal alprostadil (Caverject):
- Prostaglandin E1 (PGE1), in the vasodilator family of medications, which causes direct relaxation of vascular smooth muscle.
- via syringe into penis, store @ room temp.
- Transurethral alprostadil (Muse): a pellet inserted into urethra via plunger, refrigerate.
- SE: pain.
- Non-pharmacologic
- Vacuum cylinder SE: pain, petechiae, bruise, numbness
- Inflatable, semi-rigid, surgically implanted device
Patient education
- Identify nonessential meds that could be discontinued, for example, in case of BP disorder, change to a different class of drugs - α-adrenergic blockers and some ARB may have a positive effect on ED
- Weight loss, smoking cessation, reduced alcohol intake.
- Successful outcomes are possible only when the drug is administered at appropriate dosing intervals and with sufficient sexual stimulation.
- Patients must understand the danger of priapism and visual, hearing changes.
- Headache is common and usually is not a serious SE. Manage HA may require a lower dose of PDE5 inhibitor.
Last updated on: March 26th, 2018
Was this page helpful?
Back to top »
