3 types of dementia: Alzheimer’s disease, vascular dementia, Lewy body dementia.
Alzheimer’s: most common type, which involves neuritic plaque and tangles in the brain, interrupts neuron signaling, and ↓ acetylcholine (Ach).
Acetylcholine (Ach) is the main NT of neuromuscular conjunction for skeletal muscle (relay impulse from neuron to muscle): regulates memory, sleep, and plays a role in learning, deficiency is associated with dementia. Since it is a motor neuron, Ach is involved in muscular effects.
Presentation: memory loss. (Rule out B12 deficiency, depression, and infection)
Mainstream: acetylcholinesterase inhibitors, result in ↑Ach.
May use antidepressants for depression/anxiety management.
Delusion/anger: antipsychotics (increased risk of stroke)
Drugs
ACH-Is (acetylcholinesterase inhibitor)
Drugs: Donepezil (Aricept): ODT formula help with GI effect; rivastigmine (Exelon, patch, take with food), galantamine (Razadyne), tacrine (Cognex, not used due to hepatotoxicity)
MOA: inhibits acetylcholinesterase, the enzyme responsible for the hydrolysis of acetylcholine, results in increased ACh. Use in mild-mod AD.
SE: insomnia, GI (Nausea, give @HS/V/diarrhea)
Caution: bradycardia, drugs that lower HR, and drugs cause dizziness (beta-blockers, centrally acting alpha agonists such as clonidine, hypnotics) due to risk of dizziness and fall
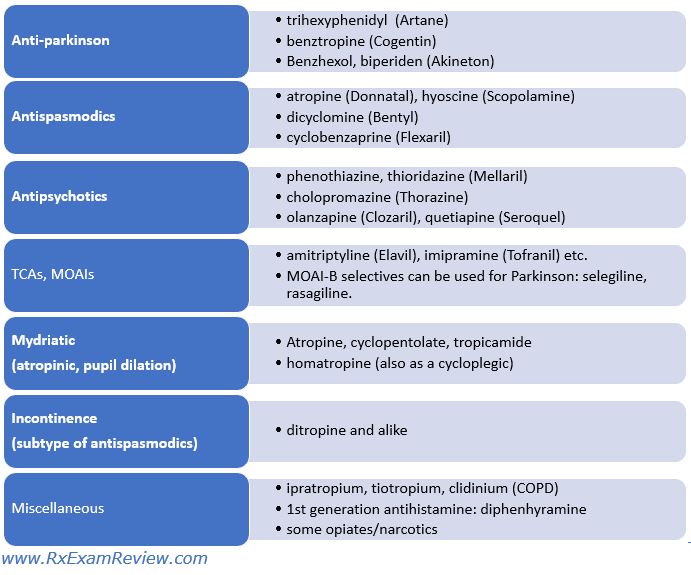
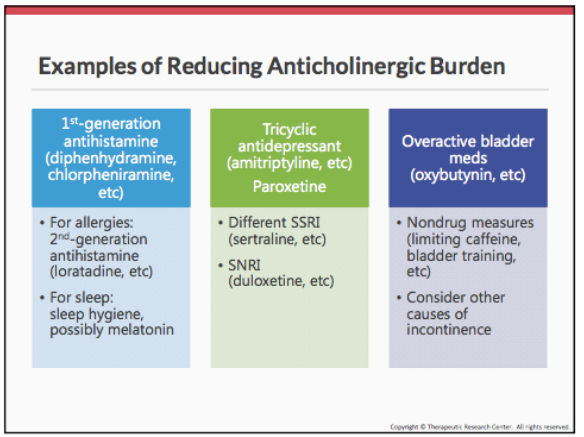
DI: drugs that have anticholinergic effects can reduce the efficacy of ACH-Is.
Memantine (Namenda)
MOA: blocks NMDA receptors (a subtype of glutamate receptor), inhibits glutamate (excitatory NT) from binding NMDA receptor, decrease abnormal activation.
Can be used alone or in combination for mod-severe AD; + donepezil = Namzaric
SE: dizziness (require dose titration)
Quiz
1. The most significant non-modifiable risk factor for developing Alzheimer’s disease is:
Presence of the ApoE4 gene
Family history
Age
Education
2. The hallmark features of Alzheimer’s disease are:
Cerebrovascular infarcts and Lewy bodies
Neuro tangles and amyloid plaques
Frontotemporal lobar degeneration and mass effect
Tau plaques and cerebrovascular infarcts
3. The increasing prevalence of Alzheimer’s disease are associated with all of the following EXCEPT:
The aging baby boomer population
The increased life expectancy over the years
The overall growth of global population
Increasing exposure to environmental toxins
4. A 72-year-old female is taking the following medications: lisinopril 10 mg QD, atorvastatin 20 mg QD, acetaminophen 500 mg every 4 to 6 hours PRN, venlafaxine 150 mg QD, and oxybutynin 10 mg QD. Which medication could worsen her symptoms of dementia?
Oxybutynin
Atorvastatin
Lisinopril
Venlafaxine
5. Which drug is NOT an acetylcholinesterase inhibitor?
Memantine
Galantamine
Rivastigmine
Donepezil
A 63-year-old female was diagnosed with mild Alzheimer’s disease and started on rivastigmine. She has been taking 1.5 mg BID for the past 2 weeks. Her physician wants to increase her dose to 3 mg BID.
6. The patient’s caregiver calls you and expresses concern that the patient is now experiencing GI discomfort. Previous to this, she had tolerated medication quite well. You should tell the caregiver:
Nausea and diarrhea tend to occur often during dosage adjustments and may subside as her body adjusts to the new dose. Taking rivastigmine with food may help.
This is a sign that rivastigmine is not the right choice and the patient should be switched to memantine.
Constipation is a common side effect of acetylcholinesterase inhibitors, and she should increase her dietary fiber.
If she cannot tolerate one medication in this class, she will not tolerate any other.
7. The patient’s GI upset continues to be bothersome despite counseling, and she is resistant to taking the medication. Her dose was reduced back to 1.5 mg BID. Her mental status remained stable (mild AD). What other option may be considered for her?
Switch to the rivastigmine transdermal patch (9.5 mg/24 hours)
Switch to the rivastigmine transdermal patch (4.6 mg/24 hours)
Switch to memantine 10 mg BID, since the patient has failed the acetylcholinesterase inhibitors.
Start scopolamine 1.5 mg patch behind the ear to help control her GI symptoms
8. Potential opportunities for healthcare savings with emerging drugs are:
Treatments that slow the rate of functional decline in AD
Treatments that reduce behavioral and psychological symptoms
Treatments that delay the onset of AD
All of the above
1: C. Age is the most significant non-modifiable risk factor for developing Alzheimer’s disease, family history and presence of the ApoE4 gene are less significant non-modifiable risk factors. Education is a modifiable risk factor.
2: B. Neurofibrillary tangles and amyloid plaques.
3: D. Environmental toxins are not associated with AD.
4: A. Oxybutynin is highly anticholinergic and readily penetrates the CNS.
5: A. Memantine is an NMDA receptor antagonist. Donepezil, galantamine, and rivastigmine are all acetylcholinesterase inhibitors.
6. A. Nausea and diarrhea are common side effects of acetylcholinesterase inhibitors. Memantine is not approved for the mild stage of AD, it is for more severe form of AD. Constipation is not commonly associated with acetylcholinesterase inhibitors. If she cannot tolerate rivastigmine, she may tolerate other medications or formulations.
7: B. Patients on total rivastigmine doses less than 6 mg can be started on the 4.6 mg patch. Patches should be changed daily and should only be applied to the lower/upper back, upper arm, or chest. Other medications/formulations from this class may be considered. Memantine is only approved for severe AD; when memantine is initiated, it should be titrated from a beginning dose of 5 mg daily. An anticholinergic drug such as scopolamine could worsen her cognitive symptoms.