Updates:
Jan 4th, 2022
Oct 26th, 2020
May 9th, 2020
Background
Blood osmolarity: higher osmolarity, more water goes into blood, ↑ blood volume, and ↑ BP. Diseases that increase blood cells ↑ BP.
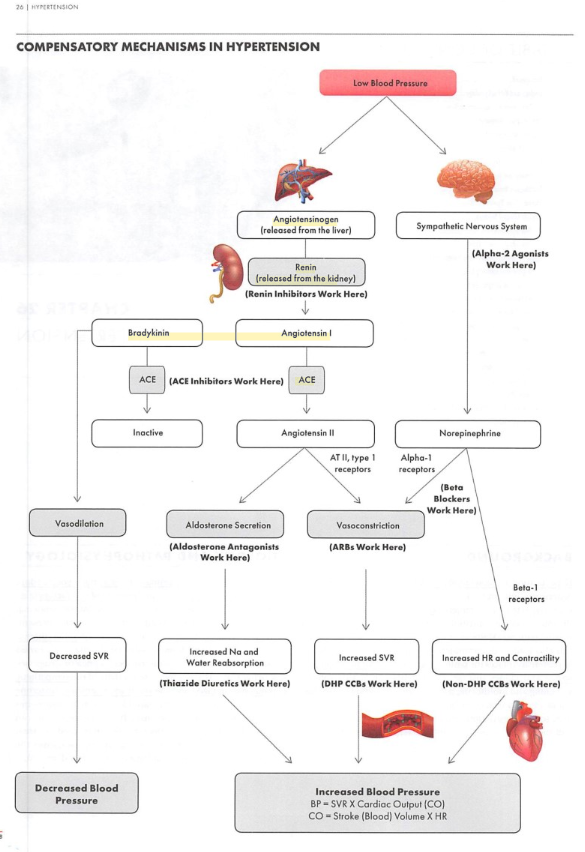
If the blood pressure (BP) is too low:
Renin-angiotensin pathway: kidney releases renin, triggers formation of angiotensin II, stimulates release, to raise BP.
Aldosterone (AKA mineralocorticoid): released by adrenal gland, causes kidney (distal tubules) to reabsorb more Na+, in turn lead to more water reabsorption. It also regulates K+ (reabsorb Na+, excrete K+)
ADH (vasopressin) is made by hypothalamus: ↑ water reabsorption in kidney, leading to ↑ BP. Higher level of ADH can cause vasoconstriction.
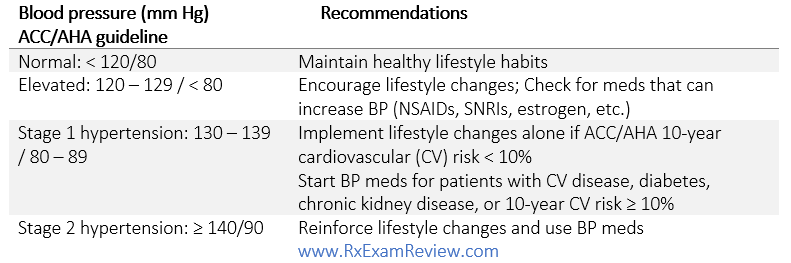
130/80 for most patients including DM (< 140/90 according to ADA, CKD, HF and elderly >=65 years old (SBP < 130)
ADA guideless is less strict with 140/90+ as the goal
Cardiovascular risk factors:
Diabetes, smoking, sex (male & post-menopause), dyslipidemia, > 60 years old, family history (male >55, female >65)
Lifestyle modification and patient education:
BMI: 18.5-24.9, DASH eating plan, less sodium in diet, physical activity 30 mins most days of week, limit alcoholic drink to 1-2 per day
Emphasize on proper technique for home BP monitoring, ask about factors that can transiently bump systolic BP: a full bladder, recent nicotine use, or talking during measurement. Ensure proper techniques such as rest for 5 mins without talking, arm supported at heart level, sit with uncrossed legs
Use a properly sized arm monitor gives the most accurate rating: Cuff that’s too small can overestimate BP, too large can underestimate BP
Wrist monitors for severely obese patients, emphasize the wrist must stay at heart level
MOA: inhibit Na reabsorption in the distal convoluted tubules of nephron (K-sparing diuretics also work here as well, but increases K, instead of lowering K).
SE: decrease (K, Mg, Na), increase (UA, LDL, TG, BG,Ca,Lithium), rash, dizziness, photosensitivity, pregnancy B. Caution: Sulfa allergy, report muscle cramps (may be caused by low K). Short term: ↑cholesterol and glucose
Good for the bones unlike loop-diuretics which cause loss of Ca.
Counsel: Take early in the day to avoid nocturia.
Patients can usually correct the mild potassium-lowering effect of thiazides by supplementing their diet with potassium-rich foods or using another antihypertensive drug to offset the effects on K-lowering (ACEI/ARB increases K).
chlorthalidone or indapamide: evidence supporting cardiovascular benefit due to longer half-life, no BP benefit at higher doses (max 25mg/day).
Not as effective when CrCl < 30 (except metolazone, use loop instead), metolazone has additional action at proximal tubule.
MOA: Work on ascending loop of Henle by blocking Na/Cl reabsorption resulting in excretion of Na/Cl/Mg/H2 Boxed warning: profound diuresis resulting in fluid and electrolyte depletion. Can be useful in GFR< 30. Preferred use in HF.
SE: hypo-K (waste more K than thiazide, requires K supplements), orthostatic hypotension, lowers Na/Mg/Cl/Ca (bad for bones), increase HCO3/metabolic alkalosis/BG/TG/TC, photosensitivity, ototoxicity (hearing loss, tinnitus, worse with ethacrynic acid), vertigo. All IV forms are light sensitive (all comes as IV), IV: PO = 1 : 2.
Caution: Sulfa allergy; ethacrynic acid is used in case of sulfa allergy, however rarely used due to ototoxicity.
K-sparing (Aldosterone antagonists & K sparing diuretics)
MOA: compete with aldosterone at the distal convoluted tubule and collecting ducts, increasing Na and water excretion while conserving K+ and H+; triamterene has a slightly different mechanism, it blocks Na channels of late distal convoluted tubules like spironolactone, but it does not compete with aldosterone. They are generally grouped together under K sparing diuretics.
Common use: HF (decrease morbidity and mortality), cirrhosis with ascites
Not effective as monotherapy and are commonly used in combination to combat thiazide’s mild potassium loss.
Black Box warning: tumor risk (spironolactone).
SE: hyperkalemia (D/C if K+ > 5.5), gynecomastia (due to androgen blocking), menstrual irregularities (due to antiandrogenic effect of the drug), hyponatremia, dehydration
Use triamterene as an alternative to avoid gynecomastia, because it does not compete with aldosterone.
DI: Li, because diuretics reduce Li renal clearance, lead to Li toxicity.
K supplements
Common use: low K, treat K-lowering side effect of diuretics.
SE: hyperkalemia (high levels of K can cause cardiac arrythmia), GI (take with food to reduce GI upset).
Oral K supplements: K-tab, Micro-K, Klor-Con.
Compensate K level by adding ACEI/ARB, K-sparing diuretics, we may get away with K supplements.
Ghost shell: patients may find the matrix shell pass out in the stool, drug is designed to leak out of the shell, counsel patients that they are getting their medication.
Sodium polystyrene sulfonate (Kayexalate), is an antidote to treat hyperkalemia; insulin is an option in emergency. (drive K intracellularly).
MOA: Angiotensin II (Ang II) is a vasoconstrictor (constricts efferent arterioles of nephron, leading to increased workload in glomeruli), and ↑ release of aldosterone, resulting in Na and water retention. Blocking Ang II can dilate efferent arterioles of nephron, leading to reduced pressure in glomeruli, therefore ACEI/ARB are thought to be renal-protective.
Role in heart failure: ACEI/ARB prevents myocardium remodeling by Ang II, therefore ACEI/ARB are 1st line in controlling BP in HF.
RAAS inhibitors should not be used in combination.
MOA: blocks the conversion of angiotensin I to angiotensin II.
SE: hypotension, angioedema (more common in black patients), hyper-K (avoid salt substitute), dry cough, dysgeusia (loss of taste), dizziness, headache. Can decrease lithium’s renal clearance and increase risk of toxicity.
ACEI/ARE is the first line therapy in many comorbidities (e.g: slow progression of kidney disease in CKD by dilating the efferent arteries of nephron; prevent cardiac remodeling in HF, stroke.
Avoid in pregnancy, angioedema, bilateral renal artery stenosis (arteries are already narrowed and would render the dilatory effect of ACEI ineffective), or with aliskiren in patients with DM or GFR <60.
Captopril: has more SE, such as neutropenia, myeloid hypoplasia, proteinuria, undesirable dosing BID-TID.
MOA: Blocks binding of angiotensin II to angiotensin receptor (AT1) sites.
SE: similar to other RAAS inhibitors but lower incidence of angioedema and cough compared to ACEIs (Mechanism is more downstream targets Ang II binding, compared to ACEI is higher up in the pathway which targets Ang I).
Direct Renin Inhibitor (DRI)
Drugs: Aliskiren (Tekturna)
MOA: Directly inhibits renin which is responsible for conversion of angiotensinogen to angiotensin I.
SE: hyper-K, hypotension, angioedema, cough, diarrhea (increase SCr and BUN); Warning: correct volume depletion prior to starting.
CI: angioedema, bilateral renal artery stenosis, do not use with ACE-Is or ARBs in patients with diabetes.
Metabolized by 3A4, be cautious on DI.
Angiotensin receptor-neprilysin inhibitor (ARNI)
Drug: valsartan/sacubitril [Entresto]
Can be used in place of an ACEI/ARB to reduce morbidity and mortality in patients with continued symptoms and heart failure hospitalizations, and maxed out with an ACEI/ARB + beta-blocker + aldosterone antagonist.
Caution with use is similar to other RAAS inhibitors.
Target dose is 97/103 mg twice daily.
Beta blockers
MOA: inhibit effects of catecholamines (hormones made by the adrenal gland, e.x: NE/epinephrine, dopamine, which are released when you are stressed), at beta-1 & beta-2 receptors to ↓ BP and HR.
Background: Adrenergic drugs mimic the activation of the sympathetic nervous system by stimulating adrenergic receptors, including alpha and beta receptors); blocking them leads to the opposite of SNS -> parasympathetic actions (vasodilation, ↓ HR).
Beta-1 receptors are primarily on the heart (1 heart), beta-2 is primarily in the lungs (2 lungs).
Not 1st line in HTN, unless the patient has comorbidity (CHF, post-MI, Afib, etc.).
SE: ↓ HR/BP, hyper/hypoglycemia, hypertriglyceridemia/decrease HDL, fatigue, dizziness, depression/decreased libido (more with lipophilic agents), most pregnancy C.
Caution in diabetes, may mask hypoglycemia EXCEPT for sweat/hunger, which occurs more often with non-selective agents (can be thought of as more powerful compared to selective agents, acts everywhere Vs specific places); one of the beta responses is increased blood [glucose] so our body can spare more energy to fight or flight, blocking the beta receptors can lead to hypoglycemia, airway disorders (beta-agonists are being used), Raynaud’s disease, aggravate psychiatric conditions (lipophilic ones can contribute to this).
DI: beta-blockers enhance hypoglycemic effects of insulin, and mask some symptoms; it can also ↓ insulin secretion, causing hyperglycemia; additive effects on ↓HR (with alpha-adrenergic agonists, non-DHP CCBs, and digoxin)
Beta-1 selective (cardio selective)
atenolol (Tenormin+ chlorthalidone = Tenoretic), acebutolol (Sectral), bisoprolol (Zebeta, + HCTZ – Ziac), betaxolol (Kerlone), metoprolol (Lopressor IR /Toprol ER IV PO), esmolol (Brevibloc IV), nebivolol (Bystolic). (A2B2MEN)
Better choice for patients with breathing problems because beta-1 receptors located only primarily on the heart.
Nebivolol has an additional pathway with nitric oxide-dependent (can be thought as more BP lowering).
Avoid in airway disease because they have effects on both airway and cardiovascular tissue receptors
Propranolol: lipophilic, and has more CNS side effects but can be useful in migraine prophylaxis and essential tremor.
Non-selective with alpha blocking effects
labetalol (Trandate, Normodyne): PO, IV used commonly in hospital, drug of choice in pregnancy.
carvedilol (Coreg): with food. Additional SE: weight gain, edema. 2D6 substrate. Can increase digoxin & cyclosporin levels; CR and IR forms are not 1:1 conversion.
More prone to causing orthostatic hypotension, but fewer metabolic effects (e.g: insulin resistance, elevation in triglycerides).
Generally avoided, especially in patients with heart failure (when HR lowing is desired), because they partially stimulate beta receptors (think about what sympathetic effects are) while blocking, and do not reduce HR to the same degree as other beta blockers.
Useful when a beta blocker is needed on board without too much HR lowering.
Calcium channel blocker (CCB)
MOA: Inhibits Ca from entering vascular smooth muscle and myocardium, causes dilation of peripheral arteries and coronary arteries.
Class effects: low BP, dose-related edema (the higher the dose, the more edema you will likely see), constipation, gingival hyperplasia.
Counsel: get up slowly to minimize risk of orthostatic hypotension.
DI: all CCB are substrates of CYP3A4 and have significant drug interactions (DI), non-DHPs are also substrates of P-gp which means even more DIs.
MOA: Inhibit Ca entry on peripheral arterial and lead to peripheral arterial dilation (compensatory mechanism of the body cause reflex tachycardia, headache/flushing and peripheral edema).
Common SE: reflex tachycardia, flushing, peripheral edema.
Clevidipine is short-acting (BP can be easily titrated), and therefore is commonly used in hospital setting for HTN emergency; Contraindicated in soy/egg allergy.
Usually dosed once daily, but you may see it dosed twice daily if the provider feels the effects wean off.
MOA: stimulate alpha-2 centrally in the brain resulting in reduced sympathetic outflow of norepinephrine (more parasympathetic effects). Since alpha receptors are not stimulated in peripheral like the systemic alpha agonists, this will not cause hypertension.
SE: ↓HR, hypotension, somnolence/headache/fatigue/dizziness, dry mouth/constipation, depression/behavioral changes/psychotic reactions/ sexual dysfunction, worsening of Parkinson's; Warning: avoid methyldopa with MAOI.
Methyldopa additional SE: hepatitis, myocarditis, positive Coombs test (positive test means more likely to have hemolytic anemia, D/C therapy), drug-induced fever, drug-induced lupus erythematosus (DILE), ↑ prolactin levels. Pregnancy safe.
Clonidine: commonly used in resistant HTN, off-label in opioid withdrawal to help nervousness, anxiety, insomnia (think about the calming/relaxing effect it may bring).
Clonidine and guanfacine can be used for ADHD.
In patients with swallow difficulty (dysphagia, dementia): Catapres-TTS patch improves adherence, it is also the only drug that comes as a patch formulation in treating high BP.
Vasodilators
MOA: These directly dilate vessels to ↓BP, unlike CCBs dilate vessels through blocking entry of Ca. The more direct effects make them more powerful.
Two main categories: non-nitrates, nitrates.
Class effects: reflex tachycardia (dose & duration dependent): compensatory mechanism of the body cause reflex tachycardia, this rule applies to all vessel dilators whether act directly or indirectly such as CCBs.)
To prevent reflex tachycardia, administer beta blocker, or an alpha-2 adrenergic agonist (e.g: clonidine, methyldopa).
MOA: Equal arterial and venous vasodilator at all doses. May increase cardiac output by decreasing afterload, and not by increasing myocardial contractility.
SE: (similar to NTG above) hypotension, tachycardia, cyanide toxicity (especially in renal and hepatic impairment), headache.
Requires protection from light during administration (wrap in foil).
Nitroprusside metabolism results in the formation of thiocynanate and cyanide which can cause cyanide toxicity (boxed warning).
High infusion rate can cause excessive hypotension, dilute solution further with D5W.
Nesiritide is a B-type natriuretic peptide (BNP), no tachyphylaxis, long half-life.
HTN urgency
BP > 180/120 without organ damage.
Oral meds with onsets of 15-30 mins, reduce BP gradually over 24-48 hrs, may repeat dose in 1-2 hrs PRN.
Drugs: Captopril, clonidine, labetalol.
HTN emergency
BP > 180/120 with organ damage (encephalopathy, MI, pulmonary edema, stroke, aortic dissection, unstable angina, intracranial hemorrhage), eclampsia (Seizure in pregnancy)
Use IV meds.: Reduce SBP/MAP within 1st hour, then to 160/100-110 over next 2-6 hrs, then to normal over next 24-48hr.
Drugs:
Clevidipine (Cleviprex, comes in lipid emulsion, discard after 4 hrs), Nicardipine (Cardene)
Vasodilators – nitrates: sodium nitroprusside (Nitropress, Nipride), nitroglycerin: will absorb into plastic, keep in glass bottle, do not use PVC tubing. Only for patients with acute coronary syndrome and/or acute pulmonary edema. Do not use in volume-depleted patients.
Enalapril IV, Hydralazine: arteriole vasodilator, Labetalol, Esmolol.
MOA: Stimulates adrenergic or dopamine receptors, they are positive inotrope (increase contraction strength).
Common Uses: shock, heart failure.
SE: increased BP, pulse changes, arrhythmia, N/V
At low doses may cause renal vasodilation; At higher doses more likely to act like epinephrine (stimulates heart and vasoconstriction – increase pulse/BP)
Usually volume replacement is first in kidney failure, but this may be used adjunct in certain situations for shock.
Alpha and beta agonist
Drugs: Norepinephrine (Levophed)
MOA: Stimulates alpha and beta receptors leading to increased BP and pulse.
Common Uses: Shock (severe hypotension).
SE: hypertension, arrhythmias, anxiety, chest pain (possible due to reduced blood flow to the heart)
Vasoconstrictors
Drug: Vasopressin (Vasostrict)
MOA: Causes an increase in cyclic AMP (numerous effects including vasoconstriction).
Common Uses: Vasodilation-related shock
Side Effects: Arrhythmia, MI, heart failure, increase BP (used for vasodilatory shock), can affect sodium levels.
Which of that following drugs may be associated with bradycardia? (Select ALL that apply)
Felodipine
Clonidine
Ivabradine
Bisoprolol
Enalapril
Which of the following drugs block both β 1and β 2receptors at low doses?
Nebivolol
Atenolol
Bisoprolol
Carvedilol
Metoprolol
A 59 year-old male patient with hypertension was started on lisinopril. He developed severe swelling of his mouth, with trouble breathing. Choose the correct statement:
The patient should be switched to Vasotec therapy.
The patient should be switched to Atacand therapy.
The patient should be switched to Lotrel therapy.
The patient should be switched to Exforge therapy.
None of the above.
A patient has high BP, but a slow HR. The patient occasionally suffers from orthostatic hypotension and syncope. The physician is concerned and does not wish to use a blood pressure medication which may lower heart rate. Choose an agent that does not significantly lower heart rate:
Nadolol
Amlodipine
Diltiazem
Verapamil
Atenolol
Fred comes to the clinic for a follow up visit for his HTN and DM management. He has been taking 3 medications to control his blood pressure for a long time. Today, the pharmacist notices a butterfly rash across Frank's nose and upper cheeks. Which of the following medications is most likely to cause this side effect?
Hydrochlorothiazide
Enalapril
Hydralazine
Eplerenone
Verapamil
Mr. Bean presented to pharmacy with a prescription for Accupril 40 mg PO daily. Which of the following is an appropriate generic substitution for Accupril?
Fosinopril
Ramipril
Triamterene
Clonidine
Quinapril
What is the mechanism of action of clonidine?
Acts as an alpha-1 agonist, resulting in a decrease in NE release
Acts as an alpha-2 agonist, resulting in a decrease in NE release
Acts as an alpha-1 antagonist, resulting in an increase in NE release
Acts as an alpha-2 antagonist, resulting in a decrease in NE release
Acts as an alpha-1 and alpha-2 antagonist, resulting in an increase in NE release
Fred has been diagnosed with heart failure and was told to begin Toprol XL 12.5 mg daily. The pharmacist dispensed a 25 mg tablet and instruct the patient to cut at the score line. Which of the following statements are true regarding Toprol XL? (Select ALL that apply.)
This is an extended-release formulation and cannot be cut.
This medication can be taken without regard to food.
The dose is likely to be titrated every 2 weeks, if tolerated.
This medication should be stored in the refrigerator.
Toprol XL can be cut at the score line; they should use a tablet cutter.
Fred is a systolic heart failure patient on carvedilol 12.5 mg twice daily. To improve medication adherence, the primary physician wants to convert him to the once daily Coreg CR. What is the equivalent daily dose of Coreg CR for GT?
BCD. Bisoprolol, clonidine, and ivabradine may slower down HR (bradycardia) and/or may be associated with heart block. The non-DHP calcium channel blockers (verapamil, diltiazem) also decrease AV nodal conduction and can cause bradycardia. However, the DHP CCBs (amlodipine) have no effect on AV nodal conduction or HR. Instead, they actually cause reflex tachycardia due to the compensation mechanism. ACEIs have no effect on cardiac conduction or HR.
D. Carvedilol is a nonselective β -blocker, blocking both β 1and β 2receptors, it also has blocking effects on alpha receptors. Atenolol, bisoprolol, metoprolol, and nebivolol are considered cardio-selective β -blockers (block β 1 receptors), especially at low doses.
E. Vasotec (enalapril), Atacand (candesartan), Lotrel (amlodipine/benazepril), Exforge (amlodipine/valsartan) are either ACEI or ARB, and all carry the risk of angioedema.
B. Beta-blockers (without ISA activity) and the non-DHP CCBs are anti-hypertensive agents that lower heart rate. They can be useful in a patient with a fast heart rate. DHP CCB does not lower HR, it may actually cause reflective tachycardia.
C. Hydralazine (Apresoline) can cause lupus-like syndrome which is dose and duration related.
E. The generic name of Accupril is quinapril, fosinopril (Monopril), ramipril (Altace), triamterene (Dyrenium), clonidine (Catapres)
B. Acts as an alpha-2 agonist, resulting in a decrease in NE release
B, C, E. Toprol XL tablets have a score line and can be cut. They remain long-acting if cut only at the scoreline. They cannot be crushed or chewed. metoprolol succinate (Toprol XL): PO, IV. IV:PO ratio 1:2.5. target dose 200mg daily.
C. The conversion of immediate-release carvedilol to Coreg CR is not on a direct mg per mg basis due to the formulation. Immediate release carvedilol 12.5 mg BID = Coreg CR 40 mg daily.