Next for moderate persistent asthma: suggest a low-dose ICS + LABA (prevent more asthma attacks than increasing dose to medium-dose steroid)
· Peak expiratory flow
Stand up straight, hold meter horizontally, blow into the meter. Repeat 2x and record the highest of 3 readings
Yellow zone: take 2-4 puffs of beta2-agonist every 20-min x 3 doses. After 1-hr, if at green: beta agonist & inhaled steroid for 7-10 days, if at yellow: beta agonist & oral steroid
Red zone (<50%): take up to 3 treatments of 4-6 puffs of beta2-agonist every 20-min. take oral steroid (40-60mg, 3-10 days). Call 911 or go to ER.
· Spacer
Enhance coordination to administer inhaled med, prevent thrush and reduce cough
Binds to b-2 receptor causing relaxation of bronchial smooth muscle, can be taken right before exercise to prevent EIB (exercise induced bronchospasm)
SE: tremor/shakiness/tachycardia (epinephrine helps you to think about the stimulating effect of SABA), hypo-K & hyperglycemia (K & glucose goes opposite)
If SABA is used more than 2 day/wk, need to increase maintenance dose.
HFA produce softer and less forceful spray, patient may experience a different taste and warmer spray than CFC (D/C due to environmental concern)
Epinephrine (Primatene): should not be used due to non-beta2 selective.
BBW: increase asthma-related death, do not use LABA as monotherapy (now the BBW is gone from LABA/ICS combos, but is still in place for LABA alone without ICS)
LABA MUST be used with an inhaled steroid, since LABA alone doesn’t reduce inflammation.
Most are indicated for 12 years and above, except for a few: Serevent, Advair, Dulera, Foradil.
Mostly dosed at BID. Foil wrapped inhalers: good for 30 - 90 days after opening.
Mast cell stabilizer
Drug: Cromolyn sodium (Intal, OTC-NasalCrom)
MOA: Prevent mast cell release of histamine and leukotrienes by inhibiting degranulation after contact with allergens.
Prophylactic agent for bronchial asthma.
2 puffs QID for >2 y/o
Corticosteroid
1st line for long term therapy with persistent asthma
Singulair to prevent EIB: take 2-hrs before exercise, Singulair chewable tab contains phenylalanine (Avoid in patients with PKU).
Montelukast: QHS, substrate of 2C9; Zafirlukast: BID.
Zileuton (Zyflo)’s mechanism is slightly different as a leukotriene modifier, it is an inhibitor of 5-lipoxygenase (as verse to an antagonist at the receptor).
Zileuton CI in active liver disease, can increase concentrations of theophylline and warfarin. BID.
MOA: a methylxanthine derived from tea used for respiratory diseases (such as COPD, bronchospasm or asthma); Blocks phosphodiesterase resulting in increased cAMP, promotes release of epinephrine from adrenal cell, which causes bronchodilation, diuresis, CNS and cardiac stimulation.
Therapeutic range: 5 -15 mcg/mL, since it follows saturable kinetics (zero-order elimination), small dose results large increase in concentration. Max dose: 900mg/day
Substrates of 1A2, 3A4
Increased level due to 1A2 inhibition: oral contraceptives, zafirlukast/zileuton, acyclovir, cimetidine, ciprofloxacin, isoniazid
Decreased level by: CBZ/phenobarbital/phenytoin/primidone, rifampin, ritonavir, smoking, SJW, tipranavir/ritonavir, high protein diet, low carb diet, thyroid hormone
Theo decreases Li level due to increase renal excretion of Li.
IV aminophylline to PO theophylline: multiple IV dose by 0.8
Omalizumab (Xolair)
IgG monoclonal antibody inhibits IgE binding on mast cell and basophil.
SC at Dr office, >12 yo, 150-375mg SC q2-4 weeks
BBW: anaphylaxis reaction(applies to all monoclonal antibodies).
Tilade (nedocromil sodium)
Inhaled anti-inflammatory for the prevention of asthma.
2 puffs QID for >6 y/o
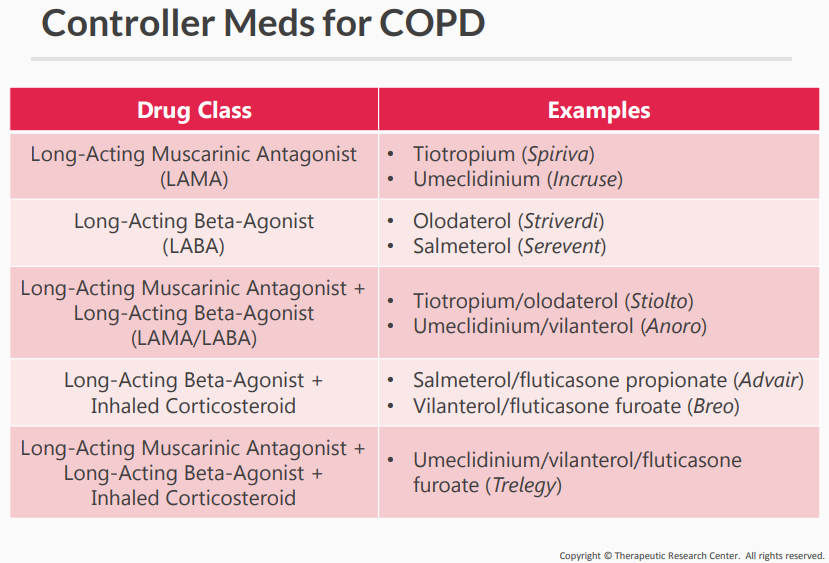
Chronic Obstructive Lung Disease (COPD)
Background
Chronic bronchitis and emphysema (destruction of the tissue of the lung), disease is not reversible.
dry-powder inhaler, single puff once daily. Reserved for patients with exacerbations on a LAMA/LABA or who also have asthma.
Daliresp (roflumilast)
A phosphodiesterase 4 inhibitor used for COPD. A CYP3A4 substrate.
500mcg po
SE: weight loss, liver impairment
Combivent Respimat instruction
Turn the clear base in the direction of the arrow until it clicks (half a turn)
Breath out slowly and fully, seal your lips around the mouthpiece without covering the air vent. Point the inhaler to the back of your throat
Press the dose release button and inhale the mist
Spiriva Handihaler
Breath out and away completely. With the handihaler in your mouth, breathe in deeply until your lung is full
You should hear or feel the capsule vibrate (rattle)
To take your full daily dose, you must inhale twice from the same capsule
Watch a short clip on how to use:
Pulmicort flexhaler
Hold the inhaler upright, twist the brown grip as far as it goes in one direction, then twist it all the way back in the other direction
Turn away from inhaler then breathe out.
Inhale the dose deeply
Foradil aerolizer
Breathe in as steadily and deeply as you can
Remove the inhaler while holding your breath for 5-10 seconds
Breathe away from inhaler.
Dry powder inhalers:
Spiriva Handihaler
Foradil Aerolizer
Diskus: Advair, Flovent, Asmanex, Serevent
Ellipt:Incruse, Anora, Trelegy
Pulmicort Flexhaler (budesonide)
Brethine (terbutaline)
It works by relaxing muscles in the airways to improve breathing.
Terbutaline is used to treat or prevent bronchospasm (wheezing, chest tightness, trouble breathing) in people with lung conditions such as asthma, bronchitis, or emphysema.