Last updated on: April 23th, 2019
Electrolyte imbalance / ICU
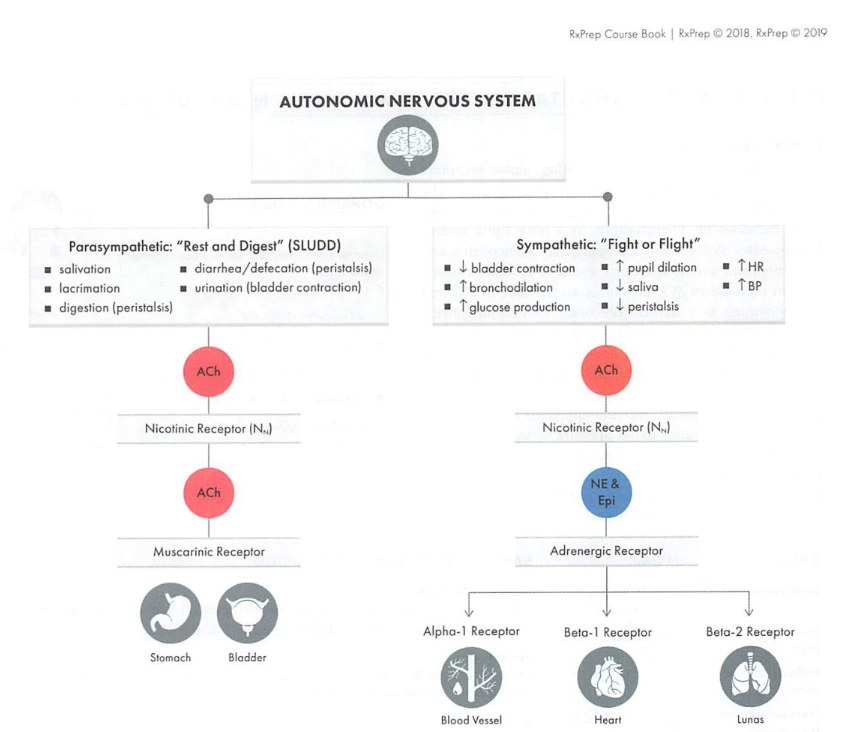
- Peripheral nervous system (PNS): somatic (controls muscle movement by releasing acetylcholine (Ach) to nicotinic receptors and autonomous (digestion, cardiac output, blood pressure)
- Autonomous system breaks down into:
- Sympathetic: fight or flight; ↑HR, BP and glucose production, by releasing NE and Epi to act on adrenergic receptors (alpha 1, beta 1 &2).
- Parasympathetic: rest and digest.
Vasopressor
- Drugs: Dopamine, Epinephrine (Adrenalin), Norepinephrine (Levophed), Phenylephrine (Neo-Synephrine), vasopressin (Vasostrict)
- MOA: Press down on vasculature causing vasoconstriction, ↑ BP
- SE: tachycardia, arrythmia, bradycardia (phenylephrine, no effect on HR), hypoperfusion and necrosis (extravasation), hyperglycemia (Epi)
- Dopamine - a precursor of epinephrine
- Epi/NE: mixed alpha and beta agonists, causing increased contractility, HR, vasoconstriction。
- Phenylephrine (Neo-Synephrine): Pure a-agonist.
- Extraversation: they are one of vesicants which cause tissue damage through extravasation. It is a medical emergency.
- To reduce risk, use central line (not peripheral), treat with phentolamine (an alpha blocker, antagonize effects of vasopressin)
- Other vesicants: vasopressors, anthracycline, vinka alkaloids (vincristine, vinblastine etc.), digoxin, foscarnet, mannitol, mitomycin, nafcillin.
Vasodilators
- Drug: Nitroprusside (Nitropress), Nitroglycerine (Nitrostat), nesiritide
- MOA: Direct vasodilation on vessel smooth muscle (arterial and venous)
- Avoid Nitroprusside in ischemic heart conditions, because it can direct blood flow away from coronary arteries.
- NTG: low dose causes venous dilation, high doses: arterial dilation.
- Nitroprusside is metabolized to cyanide and thiocyanide (hydroxycobalamin reduce risk of cyanide toxicity.
- Nesiritide: a recombinant BNP works on vascular vessel and ↑ cGMP (smooth muscle relaxation)
- CI: concurrent PDE5 inhibitor
- nitroglycerin: in glass bottle (other non-PVC options: polyolefin, polypropylene bottles)
- Sodium nitroprusside: light sensitive, wrap with foil to protect from light. Blue color sol’n indicates degradation, do not use.
Inotropes
- Drugs: Dobutamine (Dobutrex), milrinone (Primacor)
- MOA: Increase contractility through beta-adrenergic stimulation (Dobutamine) or inhibition of PDE-3 (milrinone), increase cardiac output
- SE: tachyarrhythmias
- Milrinone: selective PDEase inhibitor, not used anymore due to TCP
Fluids
- Dextrose: used when fluid is needed intracellularly, reduce content of water
- Lactated ringer (LR) or normal saline: for volume depletion.
- Iv fluids categorized into crystalloids and colloids
- Crystalloids: cheaper, fewer SE, LR maybe preferred in some states such as sepsis.
- Colloids: large molecules remain in intravascular space ↑ oncotic pressure, more expensive; albumin is commonly used in colloids, useful in severe edema (cirrhosis)
- Volume depletion: can lead to acute renal failure, and death. Signs to watch: sudden weight loss, hypotension, reflex tachycardia, acute decline in renal function, dry membranes, thirst and dizziness.
- Dehydration: both blood urine nitrogen (BUN) and serum creatine (SCr) levels increase. BUN:SCr ratio > 20:1 indicates dehydration.
- Volume overload: lead to cardiac/pulmonary complications: cardiac arrest. Signs to watch: weight gain, increased blood pressure, lung sounds (rales, crackles), and peripheral edema.
- Fluid restriction: chose the most concentrated TPN (70% dextrose, 20% lipids) and reconstitute with the least amount of fluid possible in IV.
Shock
- Characterized by hypoperfusion and hypotension ( <90/70)
- Hypovolemic: hemorrhage ; cannot give vasopressor until the volume is adequate.
- Distributive: sepsis (impaired host response to infections and life-threatening organ dysfunction), anaphylactic.
- Cardiogenic: post MI; use a positive inotrope to treat hypoperfusion, d/c any beta blockers if hypoperfusion and hypotension;
- Obstructive: embolism.
Pain
- Icu use IV fentanyl or morphine commonly.
Agitation
- Maintain regular breathing
- BZD (lorazepam, midazolam): also play a role in seizure and alcohol withdraw.
- non-BZD: propofol (Diprivan), dexmedetomidine (Precedex)
Delirium
- chose a non-BZD, usually atypical antipsychotics (e.g: quetiapine)
Stress ulcers
- H2RA and PPIs
- PPI: ↑ risk of c. diff, fracture, and nosocomial pneumonia.
Neuromuscular blocking
- Cause paralysis of muscle, commonly used in surgery. (Cholinergic agents)
- Succinylcholine (Quelicin): depolorizing agent reserved for intubation.
- Glycopyrrolate (Robinul): an anticholinergic that reduces secretion
Hemostatic agents
- MOA: causing bleeding to stop, inhibit fibrinolysis or enchance coagulation
- SE: thrombosis, vascular occlusion.
- Tranexamic acid (Cyklokapron IV, Lysteda po): Lysteda is approved for dysmenorrhea.
- Recombinant factor VIIa (NovoSeven RT)
IV immunoglobin
- For immunodeficiency conditions and other off-label use: MS, myasthenia gravis, Guillain-Barre.
- Impaired response to vaccines.
- Warning: renal dysfunction, thrombosis
Pediatric
- APGAR score: measures newborn performance in 5 categories: HR, respiratory effort, color, reflex, muscle tone. A healthy infant scores 7-10, lower score requires medical attention.
- Patent ductus arteriosus (PDA): an abnormal opening between aorta and pulmonary artery, NSAIDs (IV indomethacin or ibuprofen) is used in newborn to help it to close by blocking the prostaglandins that keep it open.
- Pulmonary hypertension: in addition to supportive care, NO is used to dilate the pulmonary arterioles, drug therapies include PDE5 inhibitors.
- Respiratory distress syndrome (RDS): is caused by deficiency in surfactant which can cause the alveoli to collapse. Newborns can receive surfactants ( “surf” or “actant” in the name), e.g: poractant alfa (Curosurf), calfactant (Infansurf).
Bacterial meningitis
- S/Sx: swelling between bones of the skull, inability to bend the neck (nuchal rigidity)
- Treatment: ampicillin + cefotaxime/gentamicin.
- Ceftriaxone is commonly used in adults but should be avoided in neonates due to hyperbilirubinemia (it can displace bilirubin from albumin and cause brain damage), it can also precipitate with Ca containing products.
Nocturnal enuresis
- Bed-wetting: is part of normal development, before age 5 does not need to be treated.
- Drug treatment: desmopressin (DDAVP, PO or nasal spray), is a synthetic anti-diuretic hormone (ADH) and ↓ urine production.
- Warnings: hyponatremia.
Pain and fever
- Avoid salicylates containing products (ASA, bismuth salicylates) in children < 16 y/o (risk of Reye’s syndrome).
- APAP infant and children’s drop are the same concentration to help reducing dosing errors (previously infant drops were more concentrated)
- Avoid ibuprofen in < 6 months old due to nephrotoxicity.
- Tylenol 10–15mg/kg PO Q4–6H
- Ibuprofen 5–10mg/kg PO Q4–6H
Gastrointestinal Issues
- Gas → Simethicone (Mylicon®) infant drops AC + QHS PRN (that’s before meals and every night as needed)
- Constipation → Pedi-Lax, MiraLax, or Glycerin suppository.
Cough and cold
- OTC products avoid in children < 4 y/o
- Avoid antihistamine in children, use nasal bulbs, saline drops instead
Drugs to avoid in pediatric
- Codeine: contraindicated in <12 y/o, can result in toxicity.
- Promethazine is contraindication in < 2 y/o, due to risk of respiratory depression.
- Quionlones: risk of cartilage, bone damage.
- Tetracycline: teeth discoloration, except in Rickessial disease doxycycline is the most effective treatment.
- Benzocaine (in topical teething gel): expose children < 2 y/o to risk of methemoglobinemia.
Quiz
- A 70-year-old female (5′ 3″, 80 kg) has a stable serum creatinine of 1.5 mg/dL. Which is an accurate assessment of her renal function?
- Stage 1 CKD
- Stage 2 CKD
- Stage 3 CKD
- Stage 4 CKD
- A 60-year-old man (5′ 10″, 92 kg) presents for annual follow-up. He has a medical history of hypertension. 2 months ago, his BP was 145/95 mmHg, serum creatinine was 1.6 mg/dL, and urine albumin:creatinine = 10 mcg:mg. Values today include: BP 145/95 mmHg, HR 84, K = 4.5 mEq/L, SCr= 1.5 mg/dL, and urine albumin:creatinine = 10 mcg:mg. Which of the following is the best recommendation?
- Chlorthalidone
- Lisinopril
- Amlodipine
- Non-pharmacological therapy only
- A female patient with stage 3A CKD and HTN presents at follow-up with a BP reading at last visit = 136/86. She began non-pharmacological therapy at that time. Vital signs today include BP 136/84 and HR 88. Labs: K = 4.2 mEq/L, SCr = 1.4 mg/dL, and urine albumin:creatinine = 100 mg:g. Which would be the best recommendation?
- Initiate chlorthalidone
- Initiate lisinopril
- Initiate amlodipine
- Non-pharmacological therapy only
- Which of the following is the most appropriate therapy in a patient with stage 4 CKD and edema?
- Indapamide
- Spironolactone
- Bumetanide
- HCTZ
- A patient with stage 3 CKD presents for a routine follow-up and has the following lab results: vitamin D 40 ng/mL, PTH 115 pg/mL, phosphate 5.3 mg/dL, Ca 9.9 mg/dL, albumin 3 mg/dL. Which is the most appropriate therapy to start at this time?
- Renagel
- Calcitriol
- Ca acetate
- Ergocalciferol
- A 32-year-old woman with hypertension, headaches, and seasonal allergies expresses a desire to become pregnant. She is currently taking methyldopa 100 mg PO daily, Zestril 10 mg daily, APAP 500 mg 1– 2 PRN Q 4– 6 hours, and loratadine 10 mg daily. Which of the patient’ s medications is a known teratogen and should be discontinued prior to conception?
- methyldopa
- Zestril
- APAP
- Loratadine
- Which of the following drugs most likely to cross the placenta?
- Highly ionized
- Highly protein bound
- Highly lipophilic
- High molecular mass (1,500 Da)
- WL is a 90 yo male with hypertension, dyslipidemia, anxiety, and seasonal allergies. His medications include clonazepam 0.5 mg PO daily, lisinopril 5 mg PO daily, loratadine 10 mg PO daily, fluticasone 50 mcg 1 spray in each nostril daily, and simvastatin 10 mg PO daily. Which of the following medications has an increased pharmacodynamic response in this patient to due to his older age?
- Clonazepam
- Fluticasone
- Lisinopril
- Loratadine
- Simvastatin
Answers
- Stage 3 CKD.This patient has an estimated creatinine clearance of 35 mL/min calculated via the Cockcroft-Gault equation. includes estimated GFR (calculated CrCl) of 15– 29 mL/min.
- Chlorthalidone. This patient’ s estimated GFR (calculated CrCl) is 52 mL/min = stage 3A CKD (45– 59 mL/min). His urine protein is <30 mcg:mg. Patients with non-proteinuric CKD have a BP goal of <140/90 mmHg and, therefore, pharmacotherapy is indicated. First line therapy for non-proteinuric is thiazide-type diuretic. An ACEI or ARB, would be appropriate first-line option for him if he had proteinuria. Calcium channel blockers are appropriate for add on therapy for hypertension.
- Lisinopril. An ACEI or ARB, would be appropriate first-line option for patients with proteinuria (>30).
- Loop diuretic is useful in low CrCl <30.
- Ca acetate is a phosphate binder that lowers PO4, and PTH. Pt’s Ca level is normal, therefore no concern for hyper-Ca.
- ACEIs are known to cause renal defects and restrict fetal growth. Methyldopa is the drug of choice in treatment HTN in pregnancy. APAP and loratadine are thought to be safe during pregnancy.
- Greater affinity for fat increases the likelihood that a drug will cross the placenta. Small molecular mass (<500 Da) agents are more likely to cross the placenta, as for drugs with lower degree of protein binding and drugs that are unionized.
- Benzos, are known to have increased pharmacodynamic effects in the elderly, and should be used with caution in older patients due to risk of cognitive impairment and fall. “LOT” are the drugs of choices.
Was this page helpful?
Back to top »
