Last updated on: Jan 14th, 2024
August 9th, 2018
Background
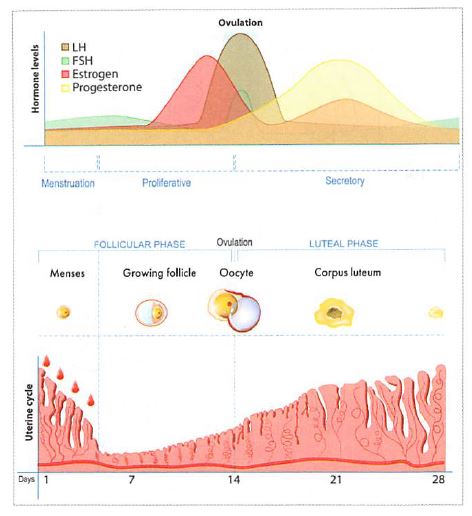
Menstrual cycle phase
- Follicular phase: Menses occur, estrogen and progesterone levels start low.
- Ovulatory phase: Surge in estrogen(E) in the mid-cycle signals luteinizing hormone (LH) and FSH (follicle stimulating hormone) to increase, LH surge triggers ovulation ( release of egg). Positive hCG+ (human chorionic gonadotropin): pregnant.
- Luteal: begins at ovulation and ends before menses. Progesterone(P) is dominant in this phase.
- E and P cause the endometrium to thicken, P causes mucus to thicken, and body temp ↑. When E and P levels are low during the cycle, spotting can occur (blood drips off the lining).
Myth on breast cancer risk
- Risk is very low after 10 years of use. Other benefits beyond preventing pregnancy: reduce endometrial /ovarian cancer risk, mitigate heavy or painful periods, etc.
- In women with a uterus, estrogen should not be used alone, this will put them at risk for endometrial cancer.
- Lower estrogen doses and different progestins in newer contraceptives are generally safer than older ones.
- In women with history of breast cancer: avoid hormonal contraception, and suggest non-hormonal options since breast cancer and clot risk increase with age. E.g.: copper IUD, diaphragm, condoms.
Estrogen/progestin combination oral contraceptive (COC)
- MOA: Inhibits (feedback inhibition) both FSH and LH, which prevents ovulation.
- SE of estrogen: Nausea, breast tenderness, bloating, weight gain, elevated BP. The lower dose is more tolerable however more spotting. If early and mid-cycle breakthrough bleeding (spotting) occurs, may require a higher estrogen dose; serious adverse effects are clotting disorder (thrombosis).
- Warnings: do not use in >35 y/o who smokes, history of clotting disorder, migraine with aura, breast/ovarian/liver cancer.
- First line for polycystic ovary syndrome (PCOS) and endometriosis, other indications: acne, dysmenorrhea, perimenopausal symptoms (PMS), anemia.
- In women with a uterus, estrogen should not be used alone, this will put them at risk for endometrial cancer.
- Women on COC have lighter periods because the endometrium remains thin.
- Start on Sunday following the onset of menses, or on day 1 of menses: if COC starts w/in 5 days of the start of the period, no backup method is needed.
- Adverse effects of estrogen: Nausea, breast tenderness, bloating, weight gain, elevated BP. If low dose/insufficient estrogen, the mid-cycle breakthrough bleeding can occur, may require a higher dose.
-
Different formulations
- Monophasic COC: same dose of hormones throughout the pack.
- Multiphasic COC (biphasic, triphasic, and quadriphasic): mimics hormonal changes during a menstrual cycle. The name of the pill can reflect the type (e.g: Tri-Previfem is triphasic, Natazia is quadriphasic).
- Extended-cycle COC (Seasonique, Seasonale): 91-pill pack with 84 active pills: Seasonale has 7-day placebo, Seasonique has 7 days of low dose estrogen; menses occur every 3 months.
- Continuous COC: Amethyst 12 months pack contains no placebo pills and no period occurs. Higher discontinuation rate due to spotting; must start within 24-hr of the start of period. Must start on Sunday, use backup birth control for the first 7 days of COC. If greater than 21 consecutive days of use, then up to 7 days can be missed, if > 7 missed doses, follow instructions for the below-missed pill during wk-1.
Contraceptive formulation
- Lo: low estrogen =< 35 mcg, and less E side effects. E.g.: Loestrin, 20mcg Vs. 35 mcg, used to reduce withdrawal symptoms and bleeding.
- Fe: with iron. E.g.: Loestrin Fe.
- 24: a shorter placebo time, 24 active pills + 4 placebo (instead of 7 placebo). E.g.: Loestrin 24 Fe.
- Ortho Evra COC patch: Backup method in 1st week of starting, change every 7 days
- Vivelle-Dot, Estradem: twice weekly patch; Climara: weekly patch
- Xulane patch: once weekly, higher systemic estrogen than pills.
- NuvaRing: Refrigeration, vaginal insert. 3 weeks in, 1 week out.
Progestin only pill (POP)
- Drugs: Camila, Errin, Jolivette, Micronor, Nor-QD, Nora-BE.
- Recommended for lactating women (estrogen reduces milk production), or for women who cannot tolerate estrogen (migraine with aura, high risk of thrombosis, etc).
- OTC norgestrel (Opill) coming soon as the first OTC daily OC pill.
- In general, POPs have fewer risks than COCs, however, they are less forgiving than COCs if a dose is missed or taken late. Important to take at the same time everyday, if 3 hrs elapsed from regular time, use a backup method.
- All come in 28-d packs, all pills are active. Start at any time, effect begins after 2 days (backup method for the first 48 hrs).
- Medroxyprogesterone (Provera) PO and inj.: a 90-day administration interval, caution on uterine bleeding irregularities.
- Adverse effects of progestin: Breast tenderness, headache, fatigue, change in mood, if late cycle breakthrough bleeding occurs, require a higher dose of progestin. Irregular menstrual bleeding is common with progestin-only pills.
Missed doses:
- COC:
- miss 1 pill: take the missed pill as soon as you remember and the next dose as scheduled, no backup is needed.
- Miss 2 pills: take as soon as you remember and the next dose as scheduled, use back up for 7 days. If the missed pills are in week 1 and 2, same as the miss 1 pill; but if in the 3rd week, after finishing this pack, skip placebos and go straight to a new pack.
- POP: if >3 hours of scheduled time, take the missed pill as soon as you remember, and the next dose as scheduled, back up for 2 days.
Drug Interactions
CYP3A4 inducers (review the list below) can reduce the efficacy of any pill, patch, or ring.
- Antibiotics (ampicillin, griseofulvin, sulfonamides, tetracycline): rifampin and its derivatives: backup method for 1.5 months.
- Anticonvulsants: barbiturates, phenytoin, etc.
- St John's wort: a strong CYP enzyme inducer.
- Anti-retroviral: HIV, hep-B meds.
- Smoking.
Therapy selection
- Breastfeeding, clotting disorder, hypertension: Progestin only.
- Estrogen side effects: Low dose estrogen
- Spotting/breakthrough bleeding: use higher estrogen/progestin if early or mid-cycle spotting, or more progestin if later cycle spotting. Wait 3 cycles before switching.
- Avoid monthly cycle: use extended formulation: Seasonale, Seasonique, Amythest (no period).
- Migraine with aura: use POP, avoid estrogen-containing.
- Fluid retention/bloating: Yasmin/Yaz (estradiol/drospirenone) or Natazia; drospirenone is a K- sparing diuretic but ↑ risk of clotting. It is also associated with less acne, due to a lower androgenic effect.
- PMS: Yaz, or antidepressant.
- Acne: COCs with lower androgenic activity (Ortho-Cyclen, Yaz, Yasmin)
- Heavy menstrual: Natazia or IUD Mirena, COC with only 4 placebos or extended regimen to ↓ bleeding.
- Mood change: monophasic COC (extended cycle or continuous is preferred).
- Nausea:take at night, or use POP, or lower estrogen dose, or NuvaRing.
- Overweight: avoid Depo-provera.
Emergency Contraception (EC)
- Levonorgestrel (Plan B): OTC no age restriction
- Ulipristal (Ella): requires a prescription, for up to 5 days of unprotected sex.
- Use a protective method until the next menstrual cycle.
- Regular OC can be started the following day after the EC dose.
Nonoxynol-9 (N-9)
- Spermicide for contraception
- N-9 should not be used to prevent HIV/STIs
Quiz
A 25-year-old woman on a monophasic COC informs you that she missed the last 2 doses of her contraceptive tablets in the first 2 weeks of the pack. In addition to using a back up method for at least the next 7 days, what would you recommend her to do?
- Take 1 extra dose today, the next dose at the scheduled time, and resume 1 tablet daily.
- Take 2 doses daily for next 2 days, then resume 1 tablet daily.
- Take 1 tablet daily until Sunday, start a new pack without taking placebo pills.
- Dispose current pack, and restart a new pack on Sunday.
Which of the following contraceptives can be used safely in a 25-year-old woman who is 12 weeks postpartum and breastfeeding her baby?
- Norethindrone/ethinyl estradiol/ferrous sulfate tablet
- Levonorgestrel/ethinyl estradiol vaginal ring
- Norethindrone-ethinyl estradiol tablet
- Norethindrone oral tablet
Answers
- B. Taking 2 doses daily for the next 2 days, then resuming 1 tablet daily is appropriate. An extra dose today, then resuming 1 tablet daily would be correct if the patient had missed only 1 dose. Starting a new pack on Sunday would be appropriate if the patient had missed 3+ doses or 2+ doses in the 3rd week.
- D. Progestin-only contraceptives are safe options during breastfeeding. Ethinyl estradiol containing contraceptives ↑ risk of clotting.
Was this page helpful?
Back to top »
