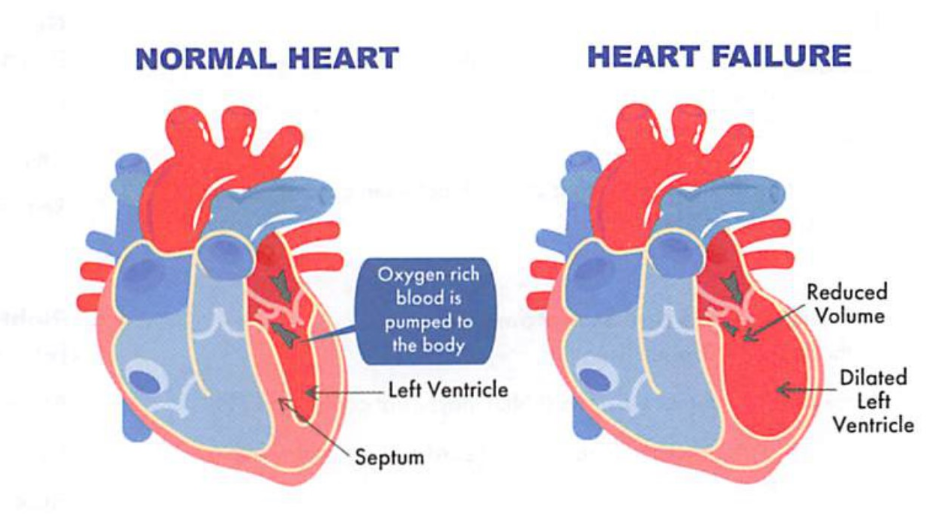
Heart failure (HF) occurs when the heart is not able to supply oxygen rich blood, due to that the ventricular failed to fill or eject blood. A weakened heart cannot provide enough oxygen and nutrients to vital organs. The body tries to compensate by stretching the heart muscle to pump better, increasing the size of the heart muscle, pumping faster; Blood vessels become narrower to keep BP up. Our body may re-route blood supply from less important areas (kidney, extremities) to more important areas (brain and heart). When these compensatory mechanisms could no longer make up for the deficiencies of the heart, the patient begins to develop heart failure symptoms.
S/Sxs: dyspnea (shortness of breath), edema (swelling), fatigue and weakness, irregular or rapid heartbeat, cough/wheezing, weight gain (fluid retention), reduced ability to exercise; symptoms are either from systolic (contraction) or diastolic (relaxation).
HF can be either ischemic: decreased blood supply (e.g: MI, CAD) or non-ischemic: uncontrolled HTN.
Left ventricular ejection fraction (LVEF): measures how much blood is pumped out of left ventricular from each contraction, it is often called EF.
EF <40%: systolic dysfunction, or heart failure with reduced ejection fraction (HFrEF).
Labs: Natriuretic peptide markers identify patients at risk of developing HF. Both beta-type natriuretic peptide (BNP, a hormone secreted by cardiomyocytes in response to heart muscle stretching caused by increased ventricular blood volume) and N-terminal pro-B-type natriuretic peptide (NT-proBNP) can be used.
Pathophysiology
It’s worthy to review the physiology of the circulatory system heart. Let’s watch a short video clip:
Right atrium collects oxygen poor blood sent into right ventricle, then right ventricle contracts and push the blood into pulmonary artery and into lungs to be replenished with oxygen
After gas exchange the oxygen rich blood travels into pulmonary vein and back into the heart via left atrium which collects the blood and pass onto left ventricle.
Left ventricle sends oxygen rich blood to the rest of body through aorta.
CO (cardiac output ) = SV (stroke volume) x HR (heart rate)
Cardiac remodeling: The heart may compensate the low CO output by temporarily stretching to hold more blood or growing thicker wall to pump harder. This led to smaller chamber inside, and weaker muscle walls.
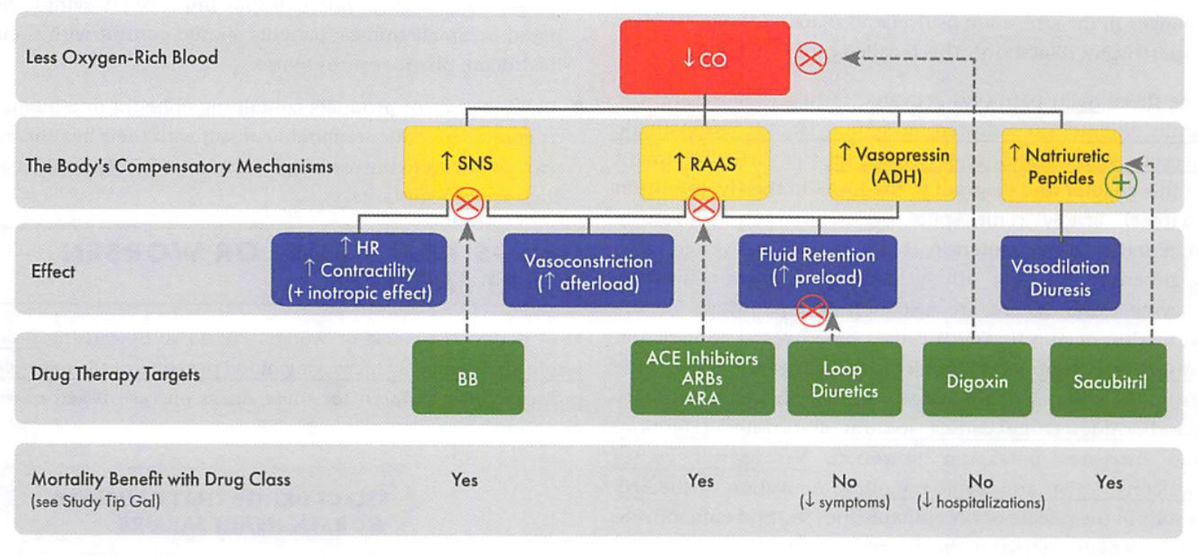
3 pathways are activated in HF: SNS (sympathetic nervous system) -> RAAS (renin-angiotensin aldosterone system) -> vasopressin.
SNS: ↑NE and epinephrine, leads to ↑ HR, contractility, vasoconstriction; causes kidney to release renin, which activates RAAS.
RAAS: releases aldosterone (↑renal reabsorption of Na and water).
Vasopressin: leads to vasoconstriction, water retention.
Furthermore, Lack of perfusion can lead to organ failure (e.g: kidney failure)
Signs and symptoms of HF
Left ventricular HF (lung): EF < 40%
Respiratory symptoms: orthopnea (SOB when at rest), pulmonary congestion, pleural effusion, cough, S3 gallop, weakness/fatigue, hypoperfusion. LV hypertrophy, ↑BNP
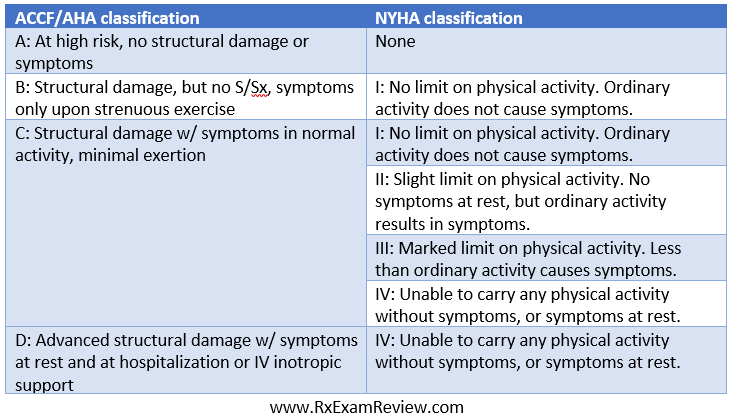
The ACCF/AHA staging system takes into account of heart abnormalities and patient risk factors. Patients do not revert to a lower stage.
The NYHA staging is classified by severity of symptoms and limitation in physical functions. (asymptomatic: A &B, symptomatic: C&D) Patients can revert to a lower classification.
Medications in managing HF
ACE inhibitors
Use with caution in patients with low BP, impaired kidney function (bilateral renal artery stenosis), or high K levels.
Elderly patients are at higher risk for ↑K, ↑ SCr, or low BP.
ARBs have a lower incidence of angioedema and cough compared to ACE inhibitors.
Beta-blockers
only carvedilol, metoprolol, bisoprolol are recommended.
They should be used in combination with an ACEI/ARB.
It may take up to 6 - 12 months to see improvement in cardiac function, counsel patients that they might feel worse when starting before they feel better.
Aldosterone antagonists
g., spironolactone, eplerenone are recommended in combination with an ACEI or ARB and a beta-blocker in select patients.
monitor K and kidney function (they work here!), make sure CrCl > 30 mL/min and K < 5 mEq/L.
eplerenone may need to be dose adjusted in patients taking 3A4 inhibitors (e.g., amiodarone, amlodipine, fluconazole, fluoxetine).
Angiotensin receptor-neprilysin inhibitor (ARNI)
alsartan/sacubitril [Entresto] can be used in place of an ACEI/ARB, in patients with continued symptoms and heart failure hospitalizations, despite maximized therapy on ACEI/ARB + beta-blocker + aldosterone antagonist
ARNIs has a slight advantage over ACEI in preventing death or hospitalizations, but causes low BP, is much more expensive, and is contraindicated in angioedema.
target dose is 97/103 mg twice daily.
Sinoatrial node modulator (ivabradine [Corlanor])
unique MOA: inhibits current in hyperpolarization, delayed depolarization -> ↓ heart rate, ↑ risk of QT prolongation. Ivabradine works primarily by lowering HR (make sure HR > 70 and normal sinus rhythm).
Option for patients who don’t tolerate beta-blockers due to hypotension, since it lowers heart rate without dropping blood pressure.
Add-on therapy in symptomatic patients with HFrEF, despite maximized therapy on ACEI + beta-blocker + aldosterone antagonist.
First new med approved for systolic HF (EF < 35%) in 2015.
3A4 substrate; Target dose: 5 mg twice daily
Diuretics:
reduce volume overload that contributes to swelling, difficulty breathing, and shortness of breath.
If volume depleted, hold dose 2-3 days; if volume overloaded, increase dose (e.g., 25%, 50%) and reassess.
Daily weights are used to monitor fluid status.
Vasodilators
Hydralazine/ Isosorbide dinitrate (Bidil) is not commonly used due to its frequent dosing and side effects
MOA: direct arterial dilator, which ↓ afterload, nitrates is a venous vasodilator, which ↓ preload. Hydralazine also reduces nitrate tolerance.
SE: HA & dizziness (from blood vessel dilation), tachycardia (compensatory mechanism the heart needs to pump faster in correspondence to vessel dilation), lupus-like syndrome (report any fever, fatigue, joint or muscle aches, more likely with larger dose over a long period of time, the symptoms will go away if stop taking it)
improve morbidity and mortality only in black patients, already receiving therapy with an ACEI/ARB, beta-blocker, and aldosterone antagonist.
Target dose: Hydralazine: 100 mg three times daily, Isosorbide dinitrate: 40 mg three times daily.
Sodium-glucose co-transporter 2 (SGLT2) inhibitors or “flozins”
dapagliflozin [Farxiga], canagliflozin [Invokana], empagliflozin [Jardiance], etc) are a class of glucose-lowering medications used to treat type 2 diabetes.
MOA: increasing the urinary excretion of glucose, as well as diuretic and blood pressure-lowering effects can benefit heart failure, improve outcomes when added to standard therapy, reduced hospitalizations.
Risks: yeast infections, hypotension, acute kidney injury, rare ketoacidosis, amputation, hypovolemia and acute kidney injury (concurrent use of diuretics); consider lower diuretic doses when starting an SGLT2 inhibitor.
Digoxin (Lanoxin, Digitek)
MOA: inhibits Na-K-ATPase pump, which results in positive inotropic effect (stronger contractility, ↑ CO) and negative chronotropic effect (↓ HR); Used for symptomatic control.
Signs of toxicity: ↓HR, arrhythmia (uneven heartbeats, PR prolongation), CNS effect (hallucinations, delirium, confusion, headache), GI (N/V, loss of appetite),; if severe, visual disturbance (blurred yellow vision, halos around light); Can become toxic if K+ is low
↓K, Mg, and ↑ Ca increase risk of digoxin toxicity.
Digoxin also has the potential to cause atrial and ventricular arrhythmias, especially with hypokalemia or impaired renal function.
Therapeutic range for HF: 0.5-0.9 ng/mL (higher range for AFib); Mostly renal cleared, reduce dose when CrCl < 30.
ACEI or ARB, beta blockers, aldosterone antagonist, ARNI (sacubril)
BiDiL: ONLY reduce mortality in African Americans.
Beta blockers: antagonize effects of catecholamines (hormones made by adrenal gland, e.x: dopamine, NE, epinephrine), BB with ISA (not enough HR lowering) should be avoided.
sacubril/valsartan: involved in several vasodilatory peptides.
Warnings: angioedema, cough, hyper-K, hypotension, do not use together with ACEI or ARB.
K-sparing diuretics (aldosterone, eplerenone): Aldosterone is non-selective, which also blocks androgen, eplerenone is selective and no endocrine effects. SE: May ↑K, TG(eplerenone), LFT, BUN/SCr; gynecomastia (aldosterone)
No morbidity/mortality benefit but improve symptoms
Digoxin, loop diuretics, ivabradine.
Meds to avoid in HF
NSAIDs
NSAID use may ↑ the risk of heart failure or worsen existing heart failure. Avoid use of NSAIDs if possible (including selective COX-2, the only advantage of COX-2 is lessened GI effects), especially in patients with HFr NSAIDs may antagonize effects of ACEI, ↑BP, promote Na and water retention, or worsen renal function.
Calcium channel blockers (CCBs)
Recommend avoiding non-DPH CCBs (diltiazem and verapamil) in patients with HFrEF, as they have a negative inotropic effect and can further reduce cardiac function. DPH CCBs are
The use of DPP-4 inhibitors in heart failure is controversial. Some evidence suggests that alogliptin/saxagliptin may increase the risk of HF. DPP-4 inhibitors appear riskiest in patients with existing heart/kidney disease.
Consider sitagliptin over alogliptin or saxagliptin. Sitagliptin appears to be the safest when it comes to risk of HF.
Amiodarone and dofetilide appear to have a neutral effect on mortality, while others have been found to increase risk of arrhythmias and should be avoided. Antiarrhythmics that should be avoided in patients with heart failure include: Dronedarone, flecainide, sotalol.
Heart failure, edema, and weight gain are side effects associated with the TZDs. These should be used with caution in patients with stable HF, and avoided in patients with symptomatic HF, and are contraindicated in patients with NYHA Class III or IV.
Triptans: CI with history of CV disease, uncontrolled HTN.
Ergo derivatives and illicit drug use: may cause heart valve disease.
Treatment of HFrEF
RAAS inhibitor is recommended for all patients with HFrEF (e.g. ACE inhibitor, ARB, ARNI).
Beta-blocker therapy should be used in combination with RAAS inhibition.
Evidence-based beta-blockers: metoprolol succinate, carvedilol, and bisoprolol.
Aldosterone antagonists (e.g., eplerenone, spironolactone) should be added in patients with continued symptoms or hospitalizations already on ACEI/ARB + BB.
Substituting an ARNI (e.g., sacubitril/valsartan [Entresto]) as a replacement for ACEI or ARB in patients that continue to have hospitalizations or significant symptoms, despite maximized therapy with BB +aldosterone antagonist.
Consider adding ivabradine in patients that remain symptomatic despite maximizing these therapies.
Consider adding hydralazine/isosorbide dinitrate to black patients that are still symptomatic receiving maximally tolerated doses of an ACE inhibitor, beta-blocker, and aldosterone antagonist
Finally, use diuretics to manage symptoms of fluid accumulation (e.g. edema, SOB).
Treatment of HFpEF
Heart failure with a preserved ejection fraction (HFpEF) is heart failure with an ejection fraction of >= 50%.
Main focus of treatment is to manage comorbidities (HTN: a risk factor for the development of heart failure, controlling BP may slow the progression of heart failure; coronary artery disease (CAD), atrial fibrillation (AFib), CKD, anemia, sleep apnea, obesity, and hyperlipidemia)
Patients with CAD and HFpEF are usually on aspirin and statin therapy.
Most patients with AFib will require rate control and anticoagulation.
Acute HF (inpatient)
Measure BNP (B-type natriuretic peptide, an important indicator of HF -), NT-proBNP in dyspnea patients
Treat fluid overload with IV loop diuretics.
Treat Low BP & CO: IV inotropics- dobutamine (Dobutrex, beta1 adrenergic agonist), milrinone (Primacor)
Treat high BP: nitroglycerin, nitroprusside
Treat high BP & low CO: nesiritide (Natrecor IV)
Patient education
Monitor body weight daily (AM before eating and after using restroom), weight gain may indicate edema and worsening of HF, notify the doctor.
Fluid Intake: Some patients may be instructed to limit fluid intake to about two liters per day in order to prevent swelling and/or shortness of breath in patients with heart failure. However, severe fluid restriction can be difficult and can also have negative effects (e.g., fluid depletion, especially if patients taking diuretics).
Quiz
Which of the following drugs is considered a positive inotrope?
Nesiritide
Nitroglycerin
Verapamil
Hydralazine
Dobutamine
Which of the following drugs has been shown to improve survival in patients with heart failure with reduced ejection fraction (HFrEF)? (Select ALL that apply.)
Digoxin
Enalapril
Ivabradine
Spironolactone
Carvedilol
Mr. Bean is a 71 year-old patient with heart failure receiving standard therapy, however, he remained symptomatic. His PCP initiated digoxin 0.25 mg QD and increased his carvedilol dose from 3.125 mg BID to 6.25 mg BID. Recent lab work shows: ALT 72 units/L, BUN 40 mg/dL, SCr 2.3 mg/dL, and K+ 4.5 mEq/L. The patient took the new medications for several weeks and started to experience nausea and a reduced appetite. He is also confused and disoriented. What is the likely cause of the patient's symptoms?
Digoxin toxicity
The increased carvedilol dose
Liver failure
Decompensated heart failure
The potassium level
Mr. Smith has New York Heart Association (NYHA) functional class III heart failure and is diagnosed with rheumatoid arthritis (RA). The physician must choose an agent to treat the RA. Which of the following medications would be the most appropriate for him?
Certolizumab
Infliximab
Methotrexate
Etanercept
Rituximab
An elderly patient with NYHA functional class IV heart failure is using 120 mg of furosemide twice daily. He takes his furosemide at 8 am and 12 noon. He has several conditions and takes a lot of pills. The prescriber requests that you calculate the dose of bumetanide that would be equivalent to the patient’s furosemide therapy. Choose the correct equivalent bumetanide dose:
Bumetanide 2 mg daily
Bumetanide 4 mg daily
Bumetanide 6 mg daily
Bumetanide 8 mg daily
Bumetanide 10 mg daily
What is correct mechanism of action for carvedilol?
Beta-1 and beta-2 blocker and dopamine blocker
Beta-1 and beta-2 blocker and norepinephrine reuptake inhibitor
Beta-1 and beta-2 blocker and alpha-1 blocker
Beta-2 and alpha-2 selective blocker
Beta-1 and alpha-1 selective blocker
A patient with systolic heart failure on digoxin has developed an upper respiratory tract infection. He has been prescribed clarithromycin. Choose the correct statement:
The digoxin level will decrease; it is best to avoid a CYP 3A4 enzyme inducer such as clarithromycin.
The digoxin level will increase; it is best to avoid a P-glycoprotein and 3A4 inhibitor such as clarithromycin.
Digoxin levels are not affected by CYP inducers or inhibitors.
Clarithromycin will bind to digoxin in the gut and reduce its absorption.
Digoxin will cause clarithromycin level to increase.
A heart failure patient is receiving furosemide 80 mg intravenously twice daily for the treatment of acute pulmonary edema. After two days, the patient is negative 3 Ls of urine output. The patient is noted to have an increasing serum bicarbonate concentration of 37 mEq/L. Which of the following agents can be prescribed to prevent development of a metabolic alkalosis?
HCTZ
Triamterene
Acetazolamide
Mannitol
Metolazone
Which of the following is a common symptoms associated with HF?
Decreased nighttime urination
Edema
Weight loss
Nausea vomiting
Which type of heart failure is associated with an ejection fraction of 40%?
HFrEF
HFmEF
HFpEF
HFtEF
Which stage of HF is associated with an EF of 35% with mild symptoms of shortness of breath and ankle edema?
Stage A
Stage B
Stage C
Stage D
what is the minimal hours for an washout period between the last dose of an ACEI and the first dose of sacubril/valsartan?
24 hours
36 hours
48 hours
72 hours
which one of the following is the most appropriate diabetes medication to add on to metformin for a patient with NYHA class III HF?
Rosiglitazone
Pioglitazone
Sitagliptin
Saxagliptin
Which electrolyte abnormality is associated with the use of salt substitute?
Low Na
High K
High Mg
Low Mg
Low K
E. Dobutamine stimulates β 1receptors in the heart and increases myocardial contractility and is therefore considered a positive inotrope. Nesiritide is an arterial and venous vasodilator. Nitroglycerin is a venous vasodilator and is used to reduce preload; it has no effect on CO. Verapamil is a negative inotrope. Hydralazine is a direct arterial vasodilator. Both drugs may increase cardiac output by decreasing afterload and NOT by increasing contractility.
BDE. ACEIs, certain β -blockers (carvedilol, metoprolol succinate, and bisoprolol), aldosterone receptor antagonists, and isosorbide/dinitrate have all been associated with a reduction in mortality in patients with HFrEF. Digoxin and Ivabradine has not been associated with a reduction in mortality.
A. The patient is likely experiencing digoxin toxicity. The patient is prescribed a dose that requires good renal function, however he has very poor renal function and digoxin is primarily (~85%) renally cleared.
: C. TNF-blockers have a warning regarding worsening or new onset heart failure; therefore, they are generally avoided in heart failure patients. Methotrexate is relatively safe for Jack.
C. Carvedilol is a non-selective beta blocker that also blocks alpha-1 receptors in arterial vessels.
B. The interaction between digoxin and clarithromycin is mainly due to the inhibition of P-glycoprotein and to a lesser extent, 3A4 inhibition.
C. Acetazolamide inhibits carbonic anhydrase, the enzyme responsible for catalyzing the conversion of carbonic acid (H2CO3) to H2O + CO2 in the renal tubule which leaves more HCO3- available for reabsorption. When carbonic anhydrase in inhibited, the reaction favors maintenance of H2CO3 which results in greater elimination of bicarbonate.
B. Edema.
A. HFrEF.
C Stage C.
B. 36 hours.
C. sitagliptin.
B. high potassium. Salt substitute replaces Na component with K.