Arrhythmia is a type of conduction disorder that is caused by abnormality in the generation or conduction of electric pulses.
Signs and symptoms include palpitation, it feels like the heart skipped a beat, or fluttering /beating too fast (tachycardia) or too slow (bradycardia), shortness of breath, and fatigue.
If the heart valves do not close fully, the blood may leak and gurgle back the wrong way (clotting risk).
Normal sinus rhtytam (NSR): originates from a SA node, which is the heart’s nature pacemaker.
The most common causes: coronary artery disease, damaged cardiac tissue, heart valve disorders, heart failure, electrolyte imbalances (K, Mg, Na, Ca), and drugs cause/worsen arrhythmia (a dangerous type torsade de pointes).
S1 sound ("lub"): tricuspid, mitral valves closing the right atrium and ventricle;S2 sound ("dub"): aortic, pulmonary valves closing the left atrium and ventricle; S3 sound (more common in heart failure) or murmurs (blood regurgitation): abnormal.
Anti-arrhythmias control the electrical conduction in heart and may also worsen the existing arrhythmia.
Types of arrythmia
Supraventricular (SVT): an umbrella term that describes arrhythmias originating from above the AV node.
Atrial flutter (F): the heartbeat originates in the atria outside the SA node, More organized than fib waves and and regular intervals, characteristic sawtooth appearance, often progresses to AFib.
PSVT (paroxysmal supraventricular tachycardia): abrupt heart rate w/ regular ventricular rhythm (a differentiation from afib).
Atrial fibrillation (AFib): absence of sinus P waves (heartbeat was not initiated from SA node), irregularly irregular ventricular response when AV node conduction is normal; P waves are replaced by fibrillatory (fib) waves.
Ventricular: originates below AV node.
PVC (premature ventricular contraction): most common arrhythmia, ventricular tachycardia and fibrillation, “skipped heartbeat”, may be related to stress, caffeine/nicotine intake.
Ventricular tachycardia (VT): a series of HR < 100.
Atrial Fibrillation (Afib)
Causes: Primary arrhythmia (idiopathic), secondary arrhythmia (cardiac or noncardiac causes).
Cardiac causes (anything related to the heart): Hypertension, Rheumatic heart disease, valve diseases, congestive heart failure, MI, etc.
Noncardiac causes (think about systemic): DM, age, obesity, hyperthyroidism, pulmonary conditions (Obstructive sleep apnea, thrombus, obstructing the flow), herbs (ephedra or ginseng, are vasoconstrictors), alcohol/drug use (usually mess up with blood flow)
S/Sx: range from asymptomatic to severely incapacitating, variable pulse pressure (irregular rhythm), hypotension (reduced CO), Fainting.
Effects: decreased cardiac output; absent atrial contraction, reduced ventricular filling during diastole. Tachycardia reduces ventricular filling time. Over time, afib with a rapid ventricular response may cause cardiomyopathy (reversible with controlled heart rate, hence why rate control is so important). Loss of atrial contraction also lead to blood stasis, which increases the risk of thrombus formation and thromboembolic complications.
management (depending on the severity of symptoms (e.g., hypotension, HF, angina)): correct underlying/contributing causes, antiarrhythmic therapy, ventricular rate control, anticoagulants, ablation, and cardioversion.
QT prolongation & Torsade de pointes (TdP)
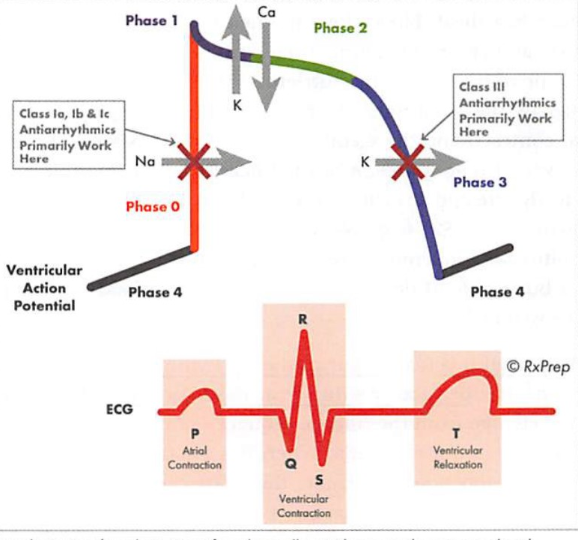
QT interval: how long it takes the heart to re-polarize after each beat. When the QT is prolonged, the heart is vulnerable to arrhythmia. QT prolongation is a marker for ventricular tachyarrhythmia and a sign of risk for the development of TdP.
Torsade de pointes: a lethal form of QT prolongation, often caused by drugs, and results in sudden death; Signs & symptoms: syncope, cardiac arrest.
Risk factors for QT prolongation and TdP: hypokalemia (diuretics etc.), hypomagnesemia, hypocalcemia, bradycardia (BB, non-DHP, digoxin, clonidine, Colanor), QT-prolonging medications (the following list), advanced liver disease (reduced CYP enzyme functions), drug interaction with CYP and P-gp. When giving a situation, you need to be able to recommend an alternative agent that does not aggravate arrhythmia.
Class Ia, III antiarrhythmics: amiodarone, disopyramide, dronedarone, procainamide, quinidine, sotalol, bretylium, ibutilide, dofetilide
DI: due to CYP systems (either 3A4 substrates, or moderate inhibitors of 2C9, 3A4 & P-gp); Reduce dose 30-50% if also on digoxin (P-gp substrate), warfarin (2C9 substrate), quinidine, procainamide; use lower dose of statins (3A4 inhibitor), and avoid grapefruit
CI: use of strong 3A4 inhibitor, drugs prolong QT, HF (class IV or hospitalization), HR < 50, CrCl < 20, hypo-K & Mg (correct electrolytes before initiating, because the primary effect is through K channels).
Class IV: non-DHPs CCBs (verapamil, diltiazem).
Patients with HFrEF should not receive it (can further ↓EF)
Amiodarone (Pacerone, Nexterone)
Long half time, lingers in body for a long time (T1/2 = 40-55 days), 200-400mg with food.
SE: hypotension, hypo/hyperthyroidism, ↑LFT, constipation, ataxia, photosensitivity, corneal deposits, blue skin discoloration, ↓HR; Known for its numerous side effects (pulmonary, hepatotoxicity); However, no effect on kidney.
BBW: lung/liver damage, exacerbation of arrythmia.
IV sol’n in non-PVC containers (polyolefin or glass), use a 0.22 micron filter.
DI: an inhibitor of many CYP enzymes, can raise level of many other drugs; need to reduce level of digoxin and warfarin; additive effects that ↓HR (BB, digoxin etc.)
Dronedarone
Less SE than amiodarone (less thyroid/ocular/QT effect and photosensitivity, but more HF
Shorter half timer (T1/2 = 13-19 hours) and less lipophilic than amiodarone
400mg BID WF
Dofetilide (Tikosyn)
Restricted prescribing and dispensing: prescribers and hospitals must enroll in Tikosyn Education program, and pharmacy T.I.P.S (Tikosynin pharmacy system), due to its BBW, and it is only initiated in a setting with continuous ECG monitoring.
MOA: slows AV node conduction to restore normal sinus rhythm.
Very short half time (t1/2 < 10s), IV access, used to facilitate diagnosis of arrhythmia (stress test of the heart).
A potent vasodilator with SE such as flushing, headache, chest pain, hypotension.
Digoxin (Lanoxin, Digitek)
MOA: decrease AV node conduction, by blocking Na-K-ATPase pump, ↓ HR ↑ contraction.
Increased level by: amiodarone, quinidine, verapamil, propafenone, spironolactone & other 3A4 inhibitors, hypo-K (K level must be maintained 3.5-5).
Decreased level by: bile binding resins, metoclopramide
DI: β blocker & Non-DHP (additive effects on heart rate).
Antidote: DigiFab.
Quiz
Which of the following carry the greatest risk of worsening arrhythmia (QT prolongation)?
phenytoin
propranolol
Sotalol
Verapamil
amiodarone
Which of the following drugs is considered a class IV antiarrhythmic?
Dofetilide
Verapamil
Flecainide
Procainamide
Metoprolol
A patient with a CrCl of 20 mL/min is brought to the ICU with a K level = 6.6 mEq/L. The EKG shows peaked T waves. She will receive treatment for hyperkalemia. Each of the following statements concerning treatment of hyperkalemia is correct EXCEPT:
Calcium IV should be given if the potassium is above 5.3 mEq/L.
Albuterol nebulized can be given stat.
If sodium polystyrene sulfonate is given, it is administered orally or rectally.
Oral and IV potassium additives should be discontinued.
Dextrose plus insulin can be given IV stat.
To help minimize the risk of QT prolongation, which antibiotic is appropriate for Mrs. King’s bronchitis?
Levofloxacin
Moxifloxacin
Amoxicillin
Clarithromycin
CE. think about class Ia, and III. Other classes are either class Ib, or class II, or class IV, are not as high risk as Ia and III.
B. The non-DHP CCBs are class IV antiarrhythmics. Dofetilide is primarily a K+channel blocker and is considered a class III antiarrhythmic. Flecainide and procainamide are Na+channel blockers and are considered class I antiarrhythmics, with flecainide designated a class Ic antiarrhythmic and procainamide a class Ia antiarrhythmic. β -blockers such as metoprolol are considered class II antiarrhythmics.
A. Calcium IV is given if the potassium is critically high and if there are EKG changes.
C. Amoxicillin. Macrolide and FQ carry risk of QT prolongation.